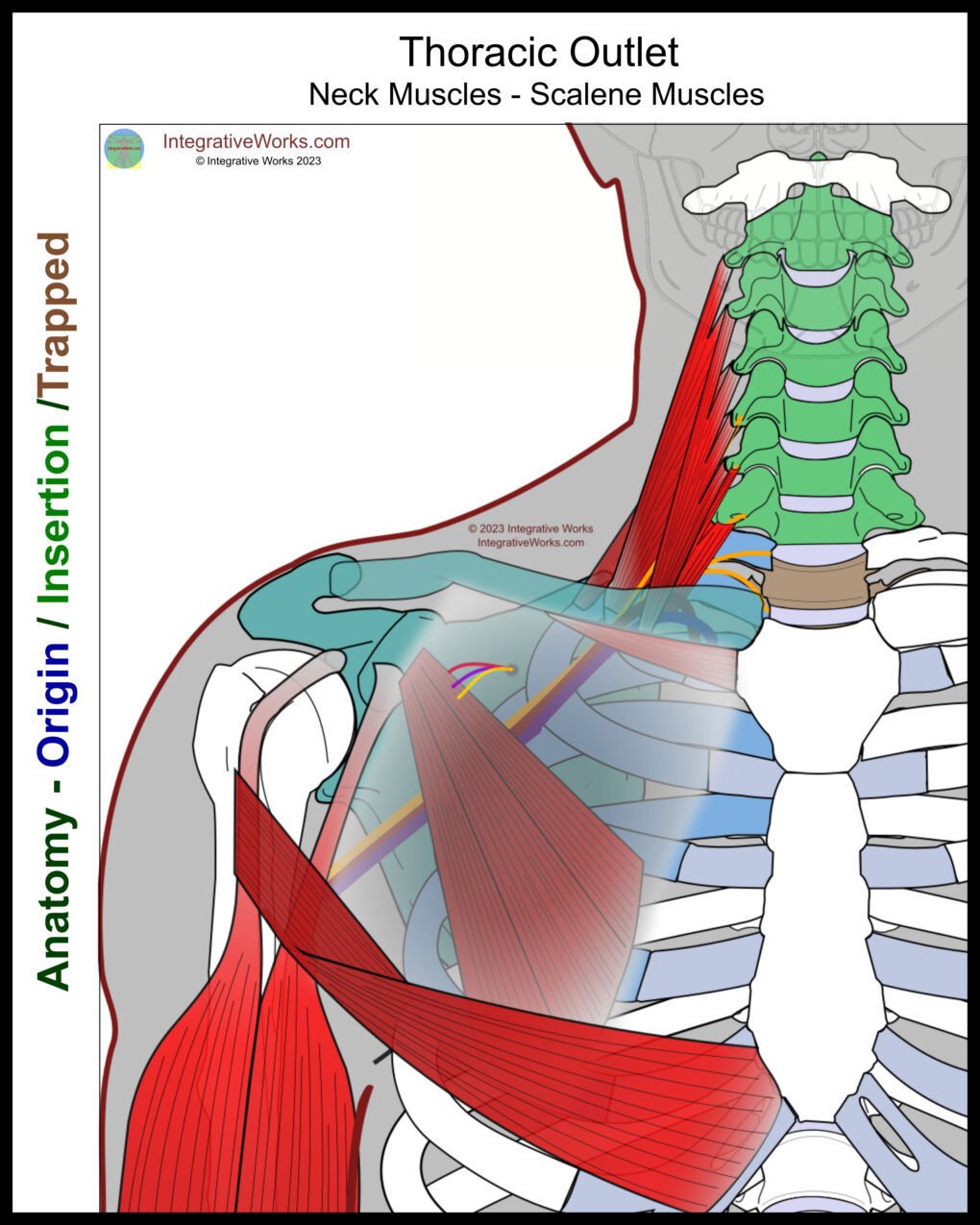
The anatomy of thoracic outlet structures is complex in several ways. First, many of the bones are both origin and insertion for muscles. Second, several of the muscles have statistically significant variations in cadaver studies. Here, you will find a brief overview of Thoracic Outlet Syndrome followed by a walk-through of the structures from back to front.
Overview
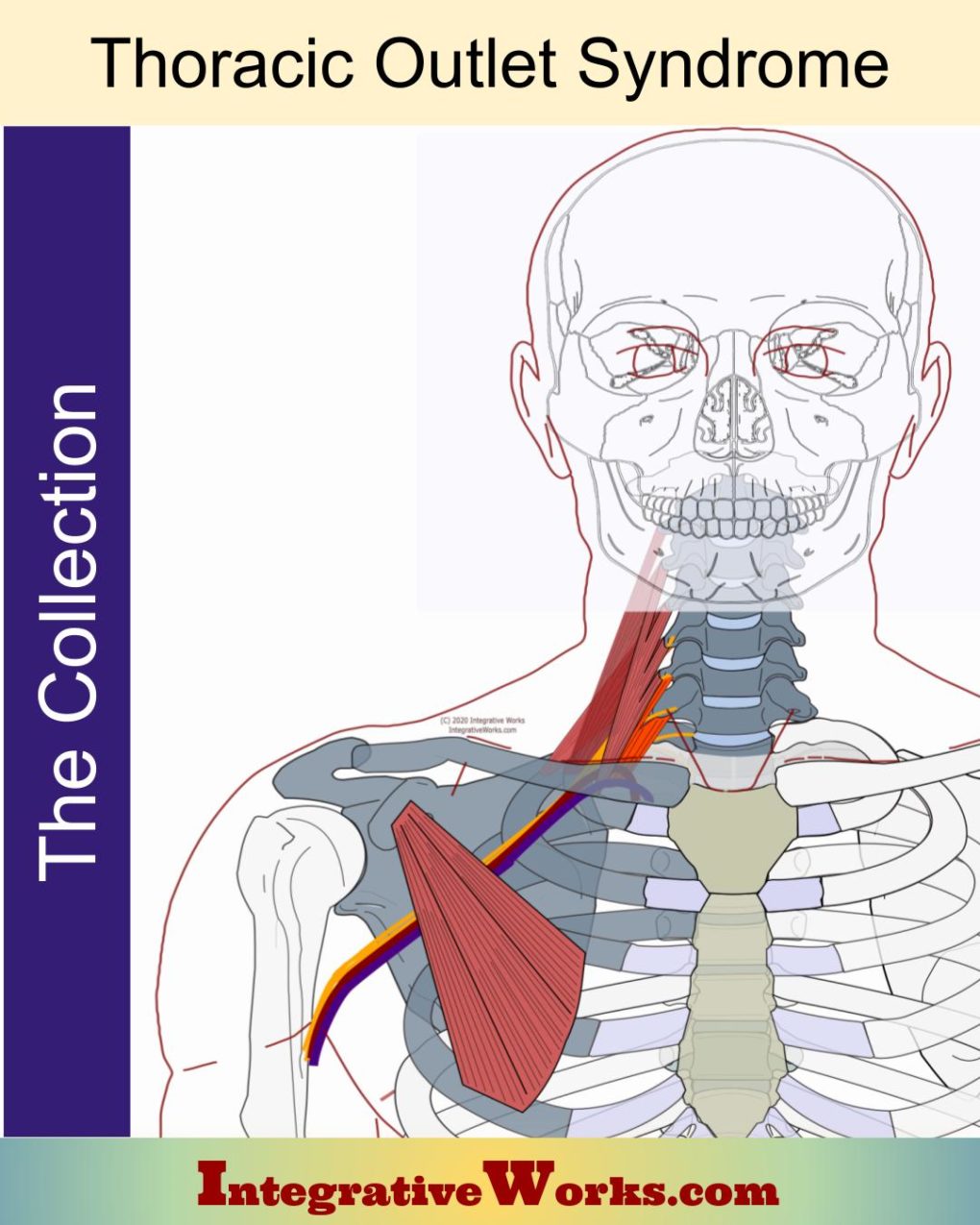
Thoracic Outlet Syndrome (TOS) is a group of related symptoms indicating a neurovascular bundle restriction that supplies the upper extremity. TOS is not a precise diagnosis. Like other syndromes, such as Chronic Fatigue Syndrome or Piriformis Syndrome, it is a collection of related symptoms.
Neurovascular Restrictions
The term “thoracic outlet syndrome” implies dysfunction occurs where the nerves and vascular structures pass over the first rib. Despite that, “Thoracic Outlet Syndrome” usually refers to structural problems impacting the neurovascular bundle from the first rib to the axilla. These problems may include restrictions in the brachial plexus, subclavian artery, subclavian vein, and subclavian lymph trunk.
The first section of this document reviews the boney structures that are most directly involved. The remaining sections examine the other involved structures, building from posterior to anterior.
Casually Speaking
Casually, people use “Thoracic Outlet Syndrome” when talking about pain and dysfunction in the upper extremity. This document focuses on the structures that create restriction and dysfunction in the neurovascular structures of the thoracic outlet.
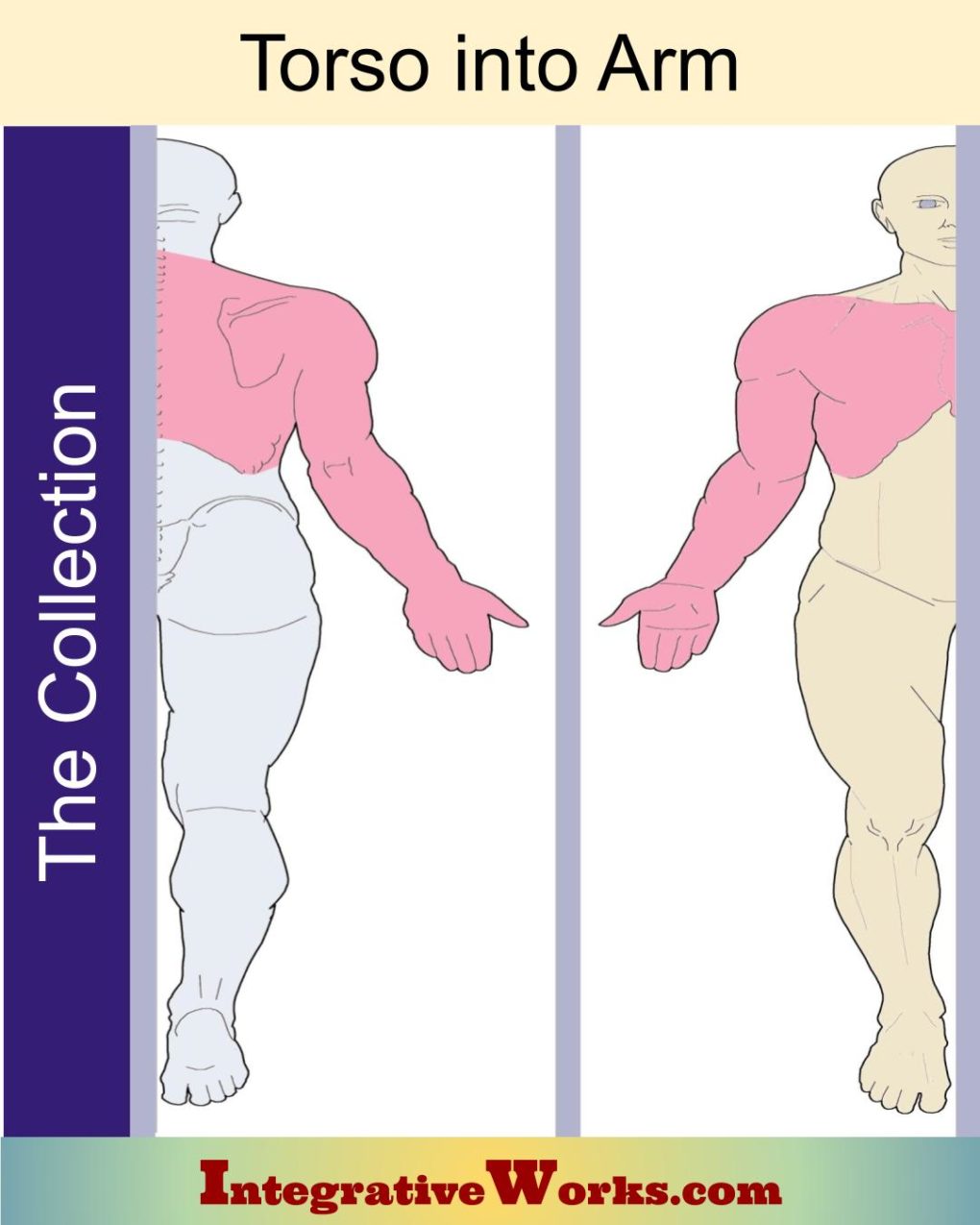
Interestingly, the muscles discussed here also have trigger point patterns that refer to the arm. In addition, several other muscles, not in the thoracic outlet structure, refer from the torso into the arm. Look at the “Torso into Arm” post for those muscles and their trigger point patterns.
Details of Thoracic Outlet Structures
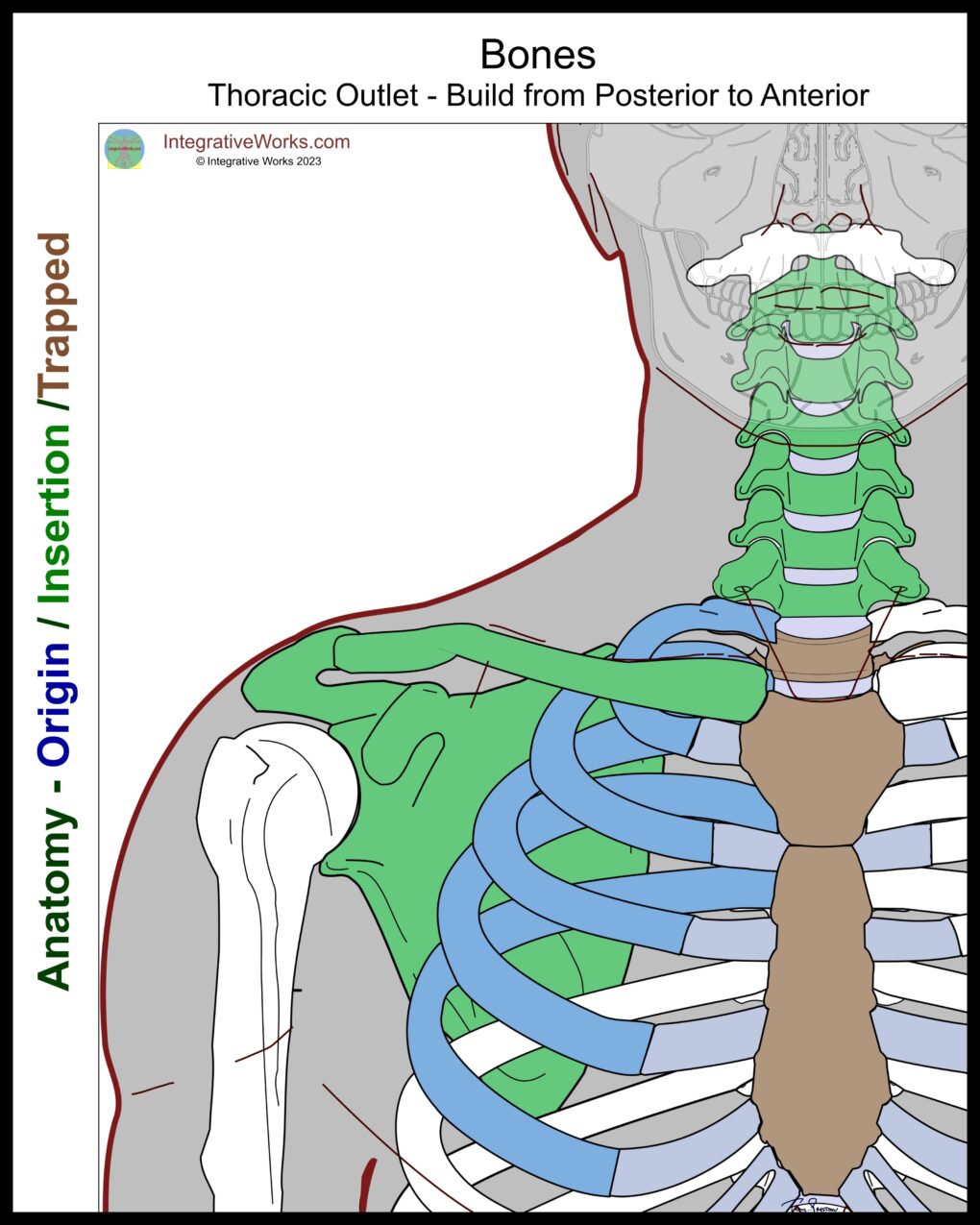
Bony Structures
Bony structures compress the nerves instead of entrapping them, creating different effects. The sensations of compression tend to feel electrical or intensely painful, like “a nail driving into the muscle.” Comparatively, entrapment of neurovascular bundles tends to create atrophy, weakness, and swelling. Trigger point referral, on the other hand, produces achy pain, sharp pain, or tingling. None of these are absolute but may be useful in a more complete assessment.
Vertebrae
C2-C7 Cervical vertebrae are particularly important in the treatment of TOS. Although radiculopathy is technically not a part of TOS, these vertebrae can compress the brachial plexus nerve roots. Further, keep in mind that balancing cervical musculature when the joints of the cervical vertebrae are binding is difficult.
Cervical radiculopathy, which often occurs from degenerative discs, technically, is not TOS. Specifically, the thoracic outlet is the ring formed by the first rib. Thoracic Outlet Syndrome happens in the structures after the plexus has formed and the neurovascular bundle comes together.
T1-T2 These two thoracic vertebrae surround the nerve roots of the lower branch of the brachial plexus (C8-T1). Forward-head posture can perpetuate TOS by causing shearing in the upper thoracic vertebrae. Displacements of the costovertebral joints of these vertebrae govern trigger points in the scalenes.
Pectoral Girdle
Clavicle When depressed, the clavicle can apply pressure on the neurovascular bundle. Padget-Schroder’s syndrome is a variation of TOS where the subclavian vein deviates medially and gets compressed between the clavicle and the first rib.
Scapula The coracoid process may press into the neurovascular bundle when the scapula has an extreme forward tilt, e.g., the pec minor is very short, and the lower trapezius is overstretched.
Ribs
First Rib –
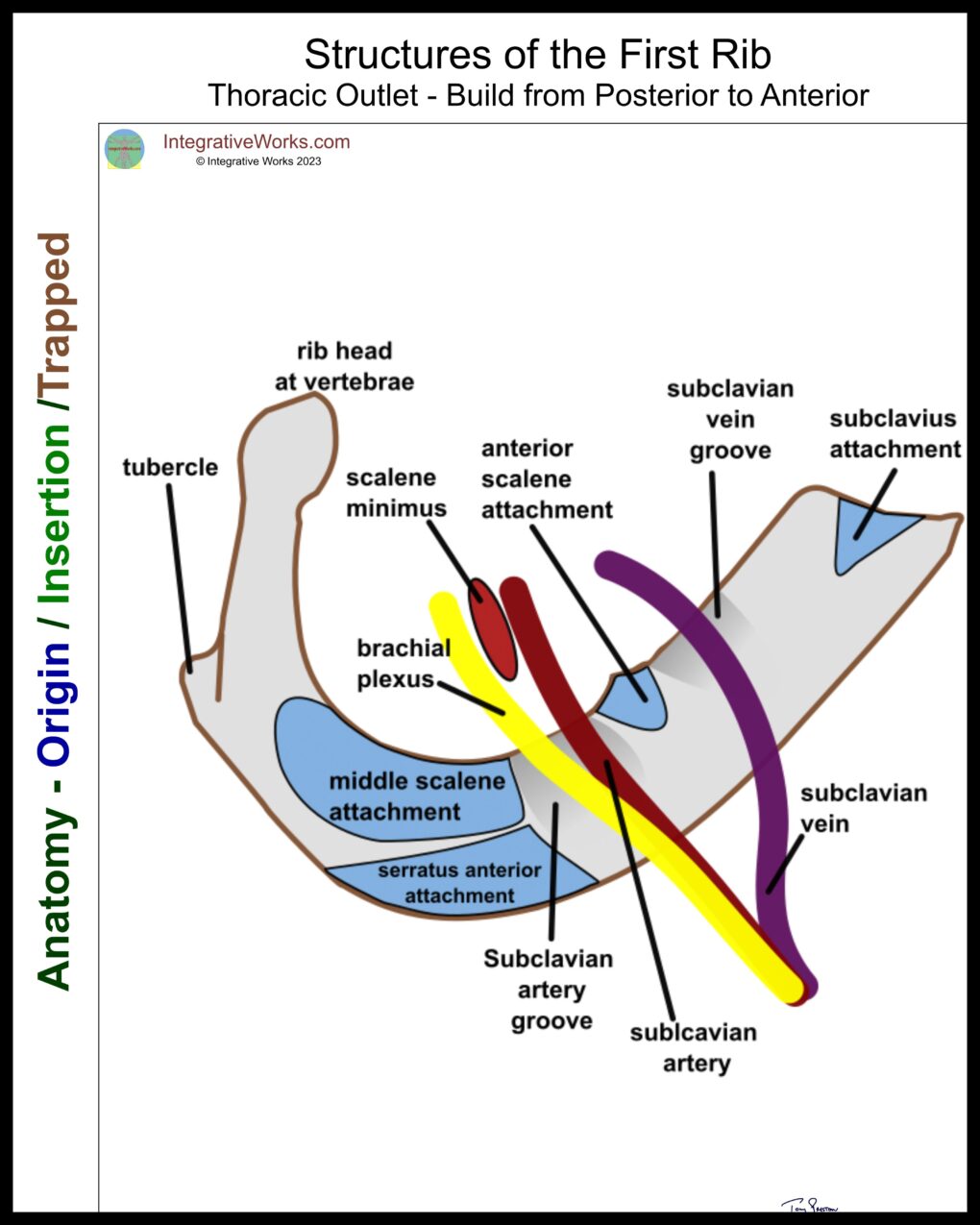
The First Rib
An elevated first rib can press into the brachial plexus. Also, proprioception from the first and second ribs governs trigger point activity in the scalenes.
Ribs 2-5 are attachments for posterior scalene and pectoralis minor – muscles that strongly contribute to TOS.
About the anatomy illustrations…
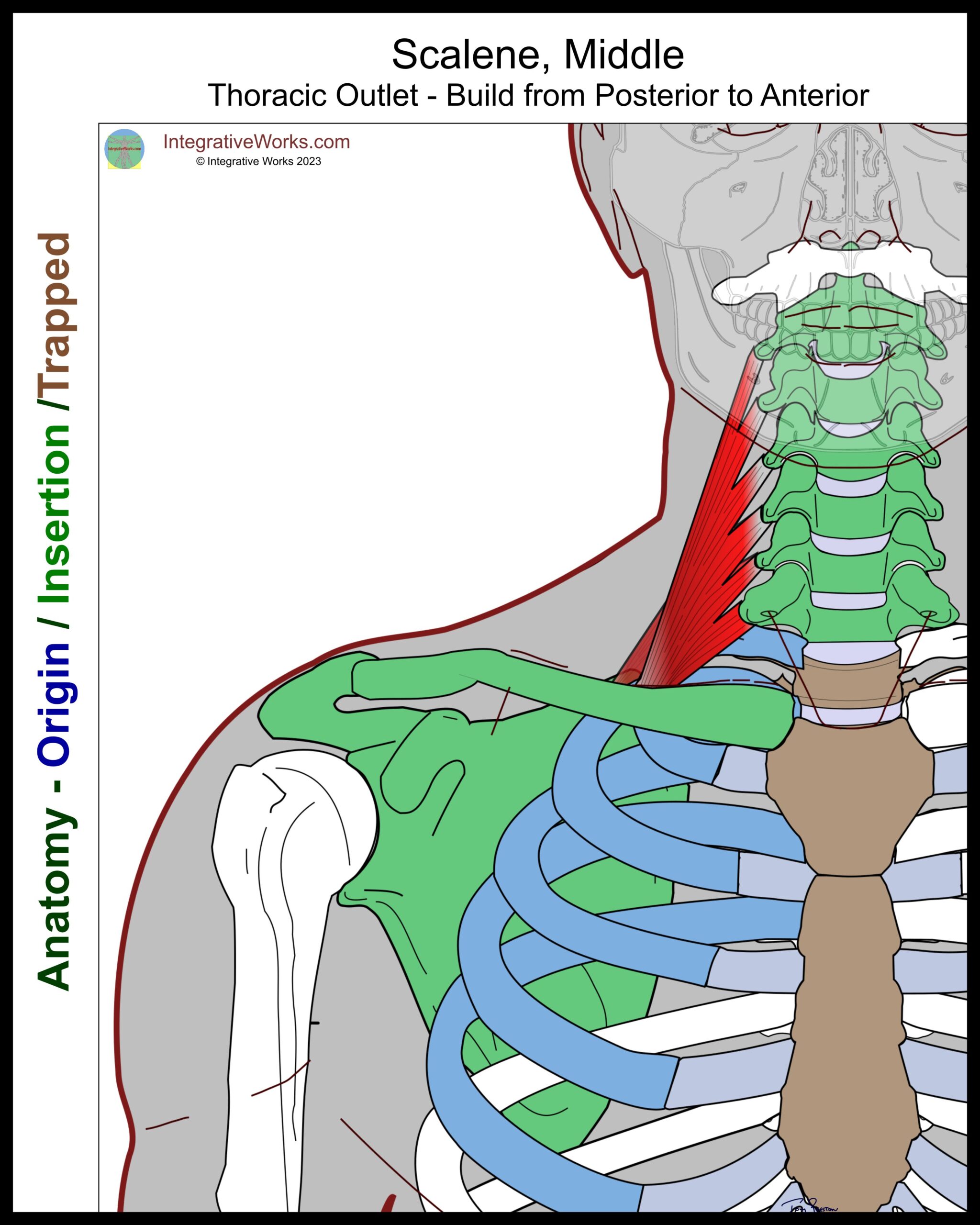
Scalenus Medius and Posticous
When concerned about TOS issues, the vertebrae are seen as the origin of these muscles.
TOS concerns
Scalene muscles pull up on the ribs, creating a couple of problems. First, they proprioceptively create trigger points in the scalenes. Next, they compress the first rib into the clavicle. In addition, the hypertrophied scalenus medius forms a larger, stiffer wall behind the brachial plexus and subclavian artery.
Scalene trigger points refer to the chest, back, shoulder, arm, and all the way into the hand. This post discusses those muscles, trigger point patterns, self-care, massage notes, and more.
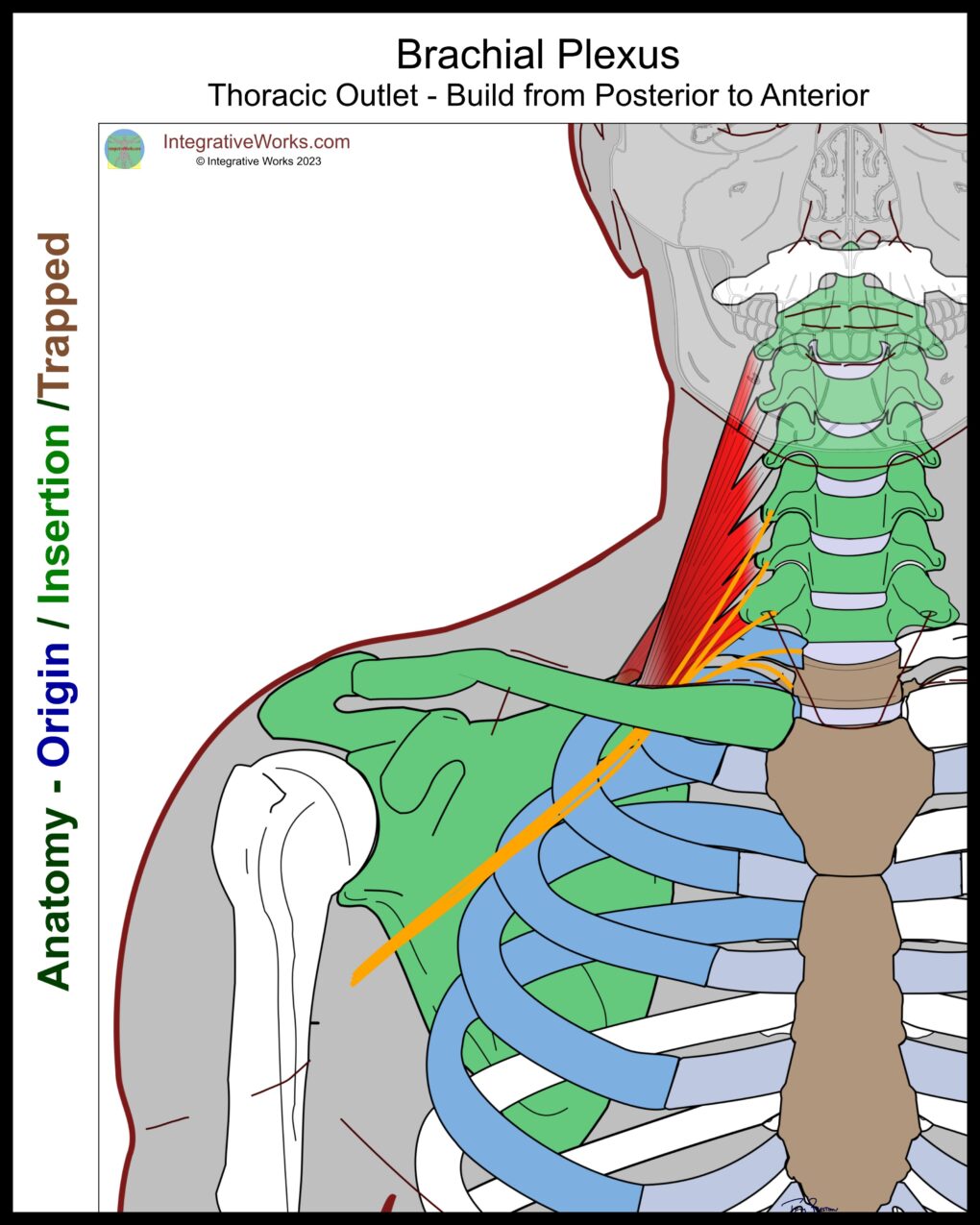
Brachial Plexus
The brachial plexus is composed of nerve roots from C5-T1. Close to the vertebrae, they form two main bundles. C5, C6, and C7 combine into the upper trunk. C8 and T1 merge into the lower trunk. These trunks form into groups before the plexus passes through the scalenes.
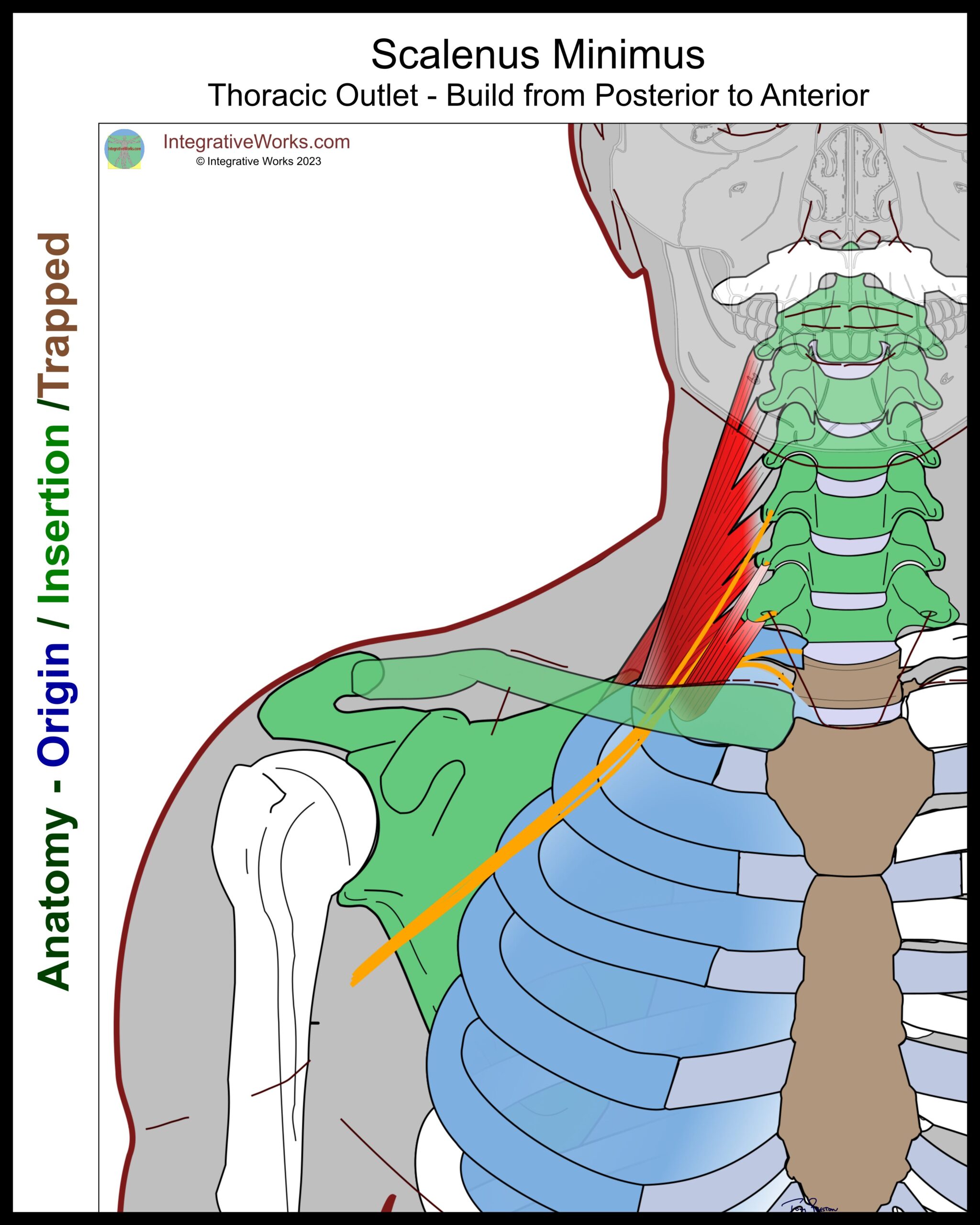
Scalenus Minimus
Scalenus minimus is a small muscle that extends from the C7 and/or C6, to the dome of the pleural fascia, which covers the chest cavity. It appears to reinforce the thick fascia that connects the anterior tubercle of C7 to the first rib.
Travell found scalenus minimus on at least one side of about half the subjects she studied. She remarks that, when it occurs, it can be a strong, thick muscle.
TOS concerns
Scalenus minimus contributes to neurovascular pressure in several ways. One, it elevates the first rib, pulling it into the clavicle. Two, it can press the brachial plexus into the medial scalene. Three, it can press the subclavian artery into the anterior scalene.
Scalene trigger points refer to the chest, back, shoulder, arm, and all the way into the hand. This post has more about those muscles, their trigger point patterns, self-care, massage notes, and more.
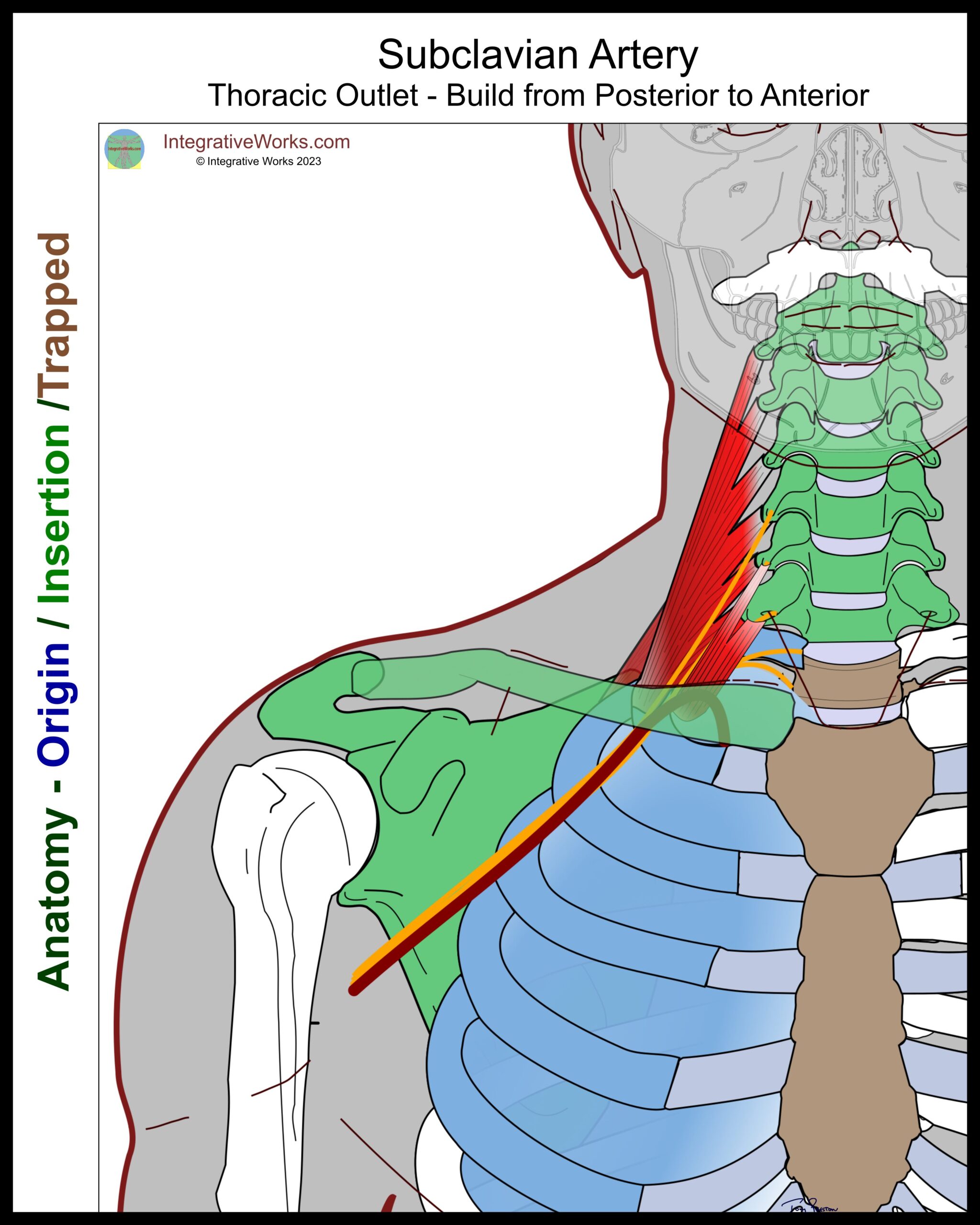
Subclavian Artery
The subclavian artery exits the thoracic cage near the mid-line and loops over the first rib. It is mostly medial and, at times, anterior to the brachial plexus as it extends toward the axilla.
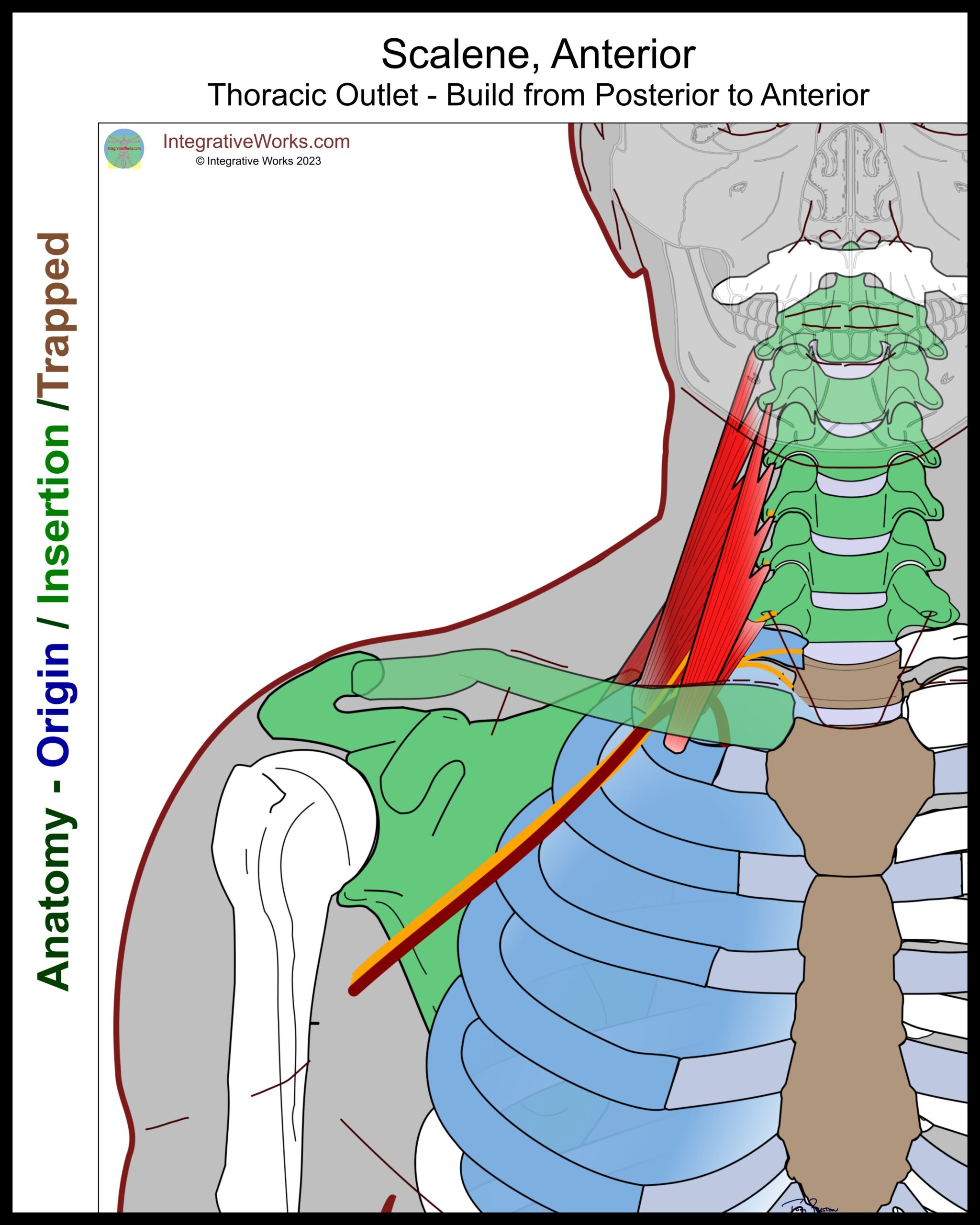
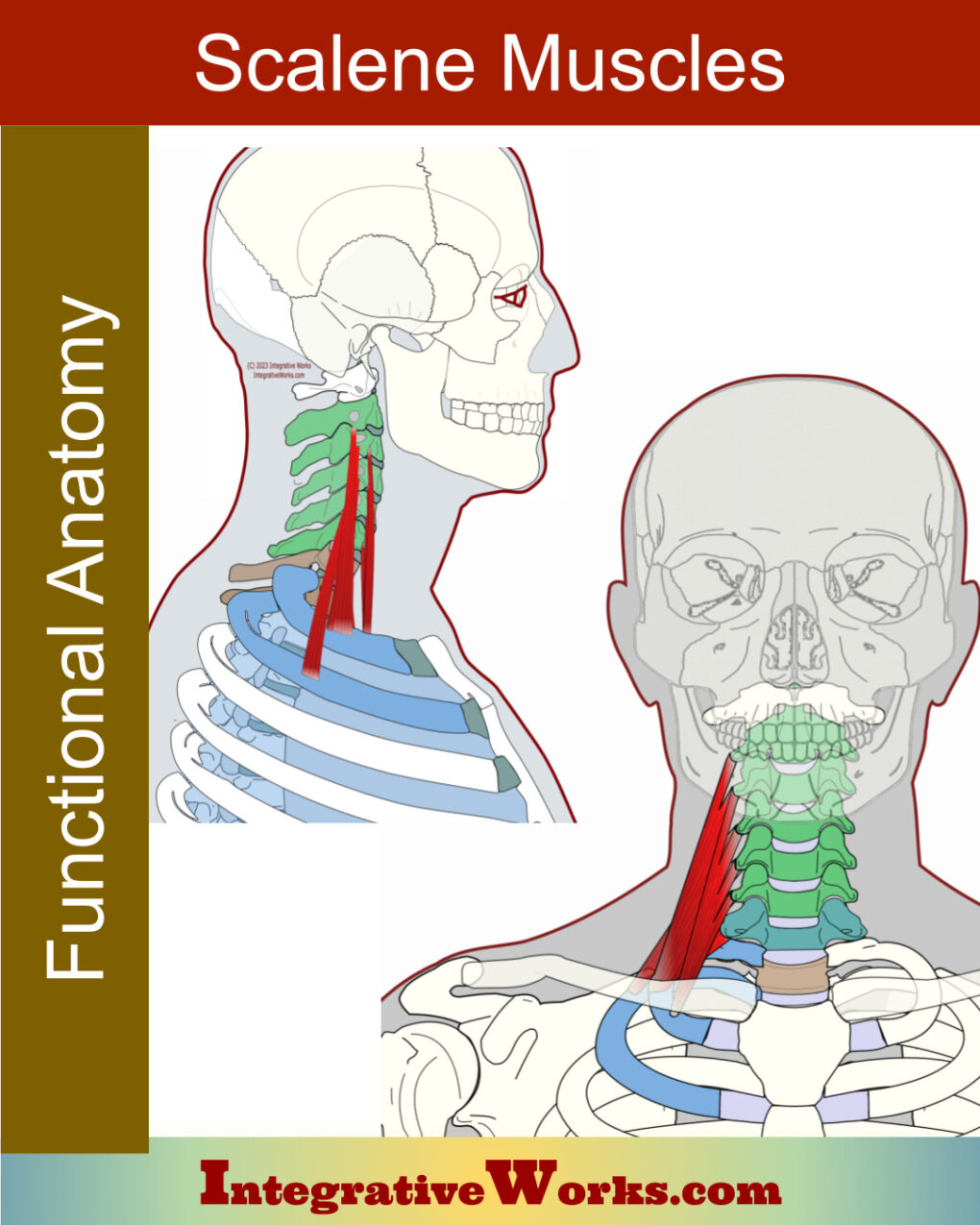
Scalenus Anticus
The anterior scalene usually attaches to the anterior tubercles of the 3rd, 4th, and 5th cervical vertebrae. This tubercle is just anterior to where the nerve roots exit.
TOS concerns
Note that the anterior scalene can press the subclavian artery and brachial plexus against scalenus medius. And, when its attachment along the 1st rib extends more posteriorly than normal, it is particularly prone to cinch on the plexus and artery. In addition, it elevates the first rib, pulling it up to compress the neurovascular bundle against the clavicle. Finally, it can press the subclavian artery into the scalenus minimus, when present.
Scalene trigger points refer to the chest, back, shoulder, arm, and all the way into the hand. This post has more about those muscles, their trigger point patterns, self-care, massage notes, and more.
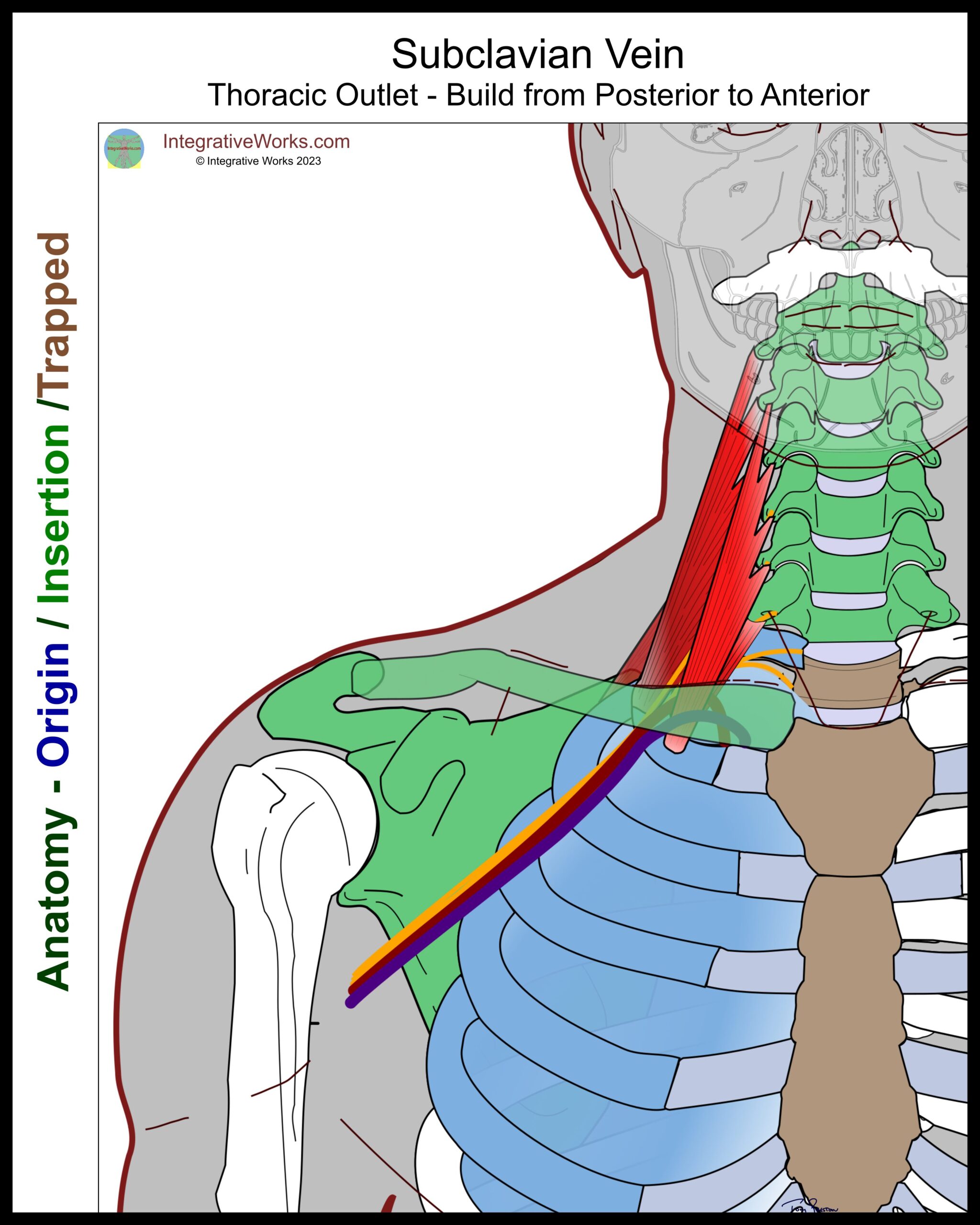
Subclavian Vein
The subclavian vein exits the thoracic cage anterior to the attachment of scalenus anticus. It travels through a groove in the first rib with the neurovascular bundle before it passes into the axilla.
Subclavian Lymphatic Trunk (not shown)
The subclavian lymphatic trunk inserts into the subclavian vein medial to the insertion of the muscles on the ribs. Some lymph vessels extending off the main trunk follow the subclavian vein and can be entrapped to restrict lymphatic flow.
Clavicle
TOS concerns
When depressed, the clavicle can apply pressure on the neurovascular bundle. At times, this happens when the first rib elevates. In other cases, it occurs when the shoulders are depressed and retracted by extrinsic back muscles.
Paget-Schrotter’s Syndrome is a variation of TOS where the subclavian vein deviates medially and gets compressed between the clavicle and the first rib. Often, It is treated with blood thinners and, eventually, surgery to resection the rib.
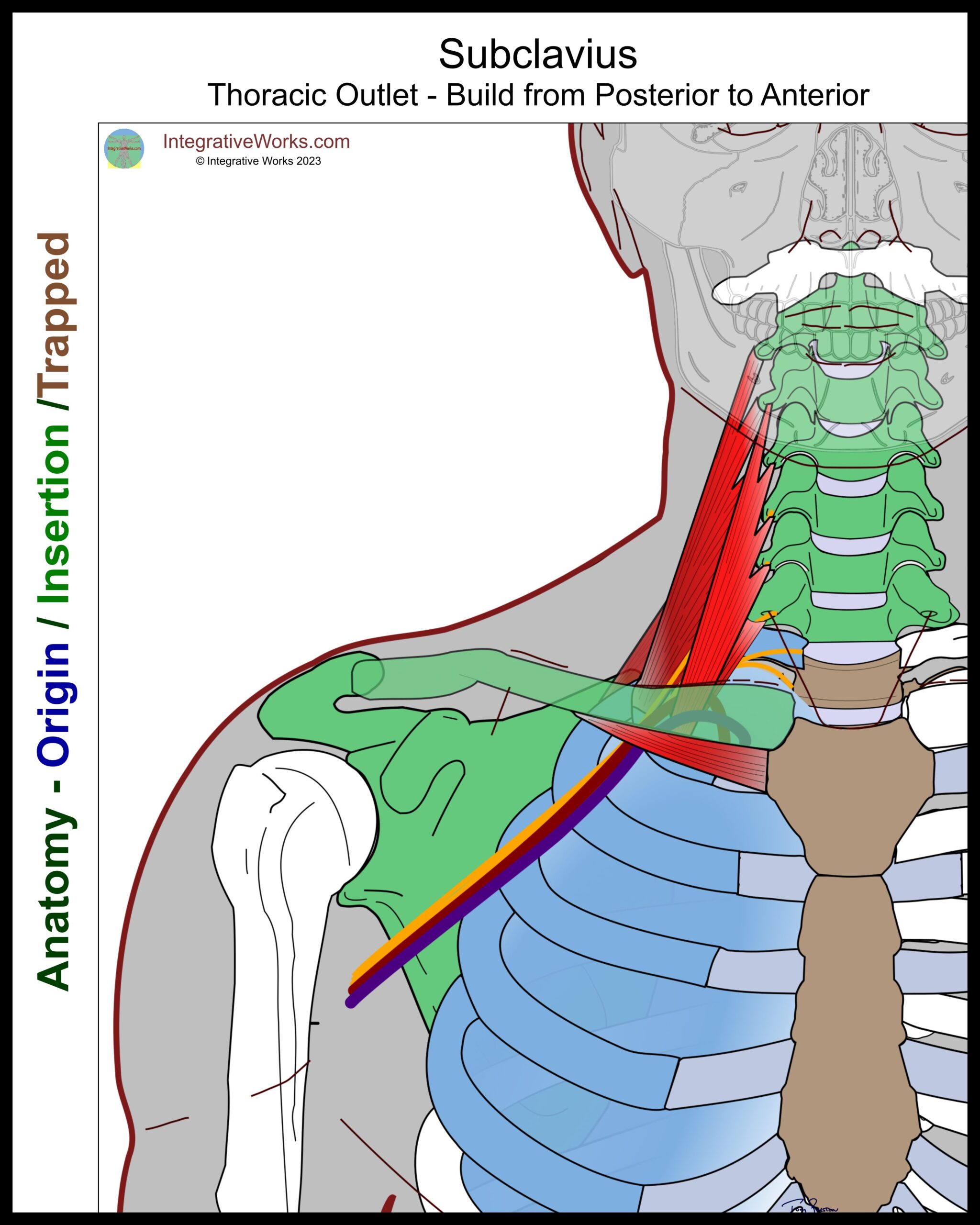
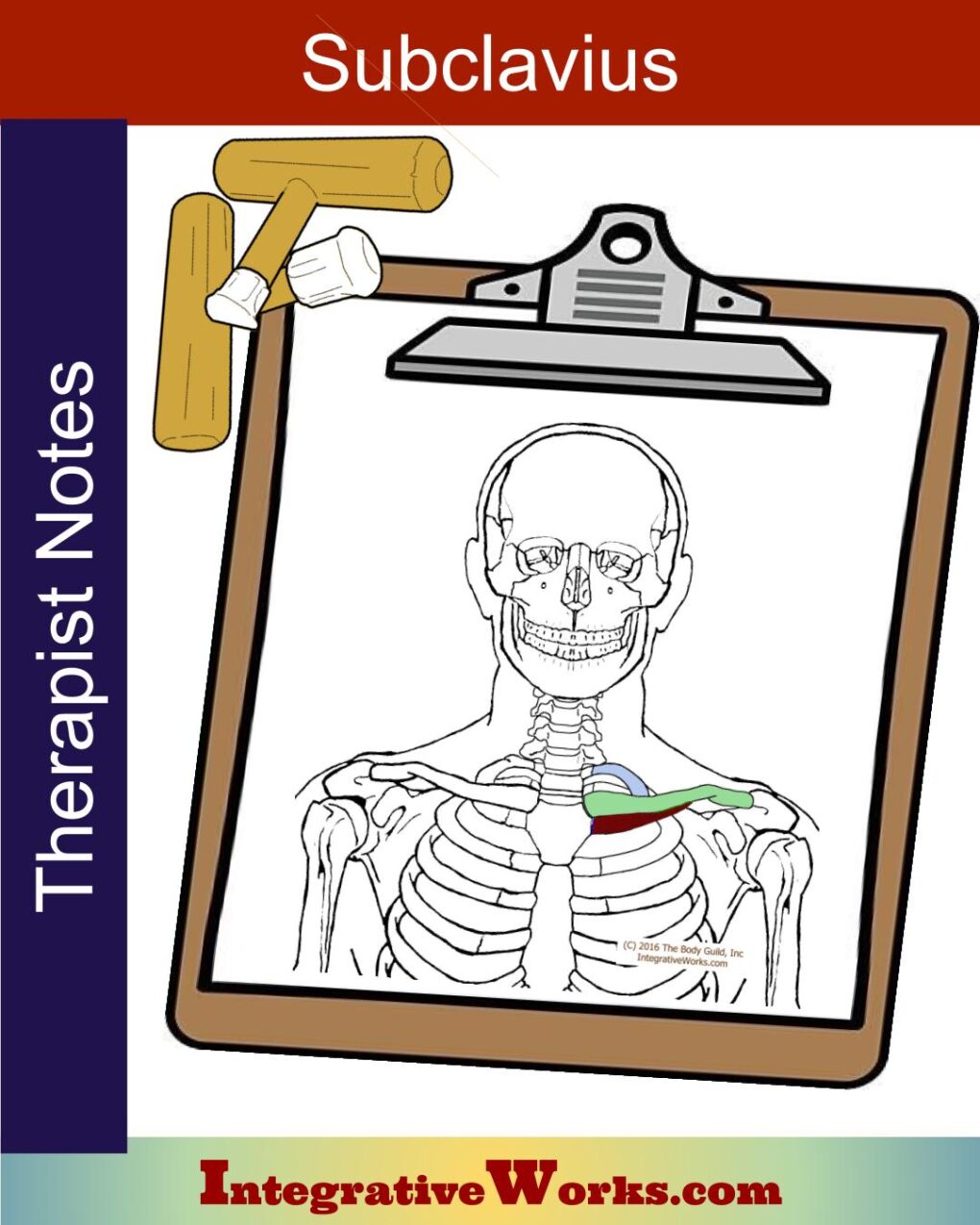
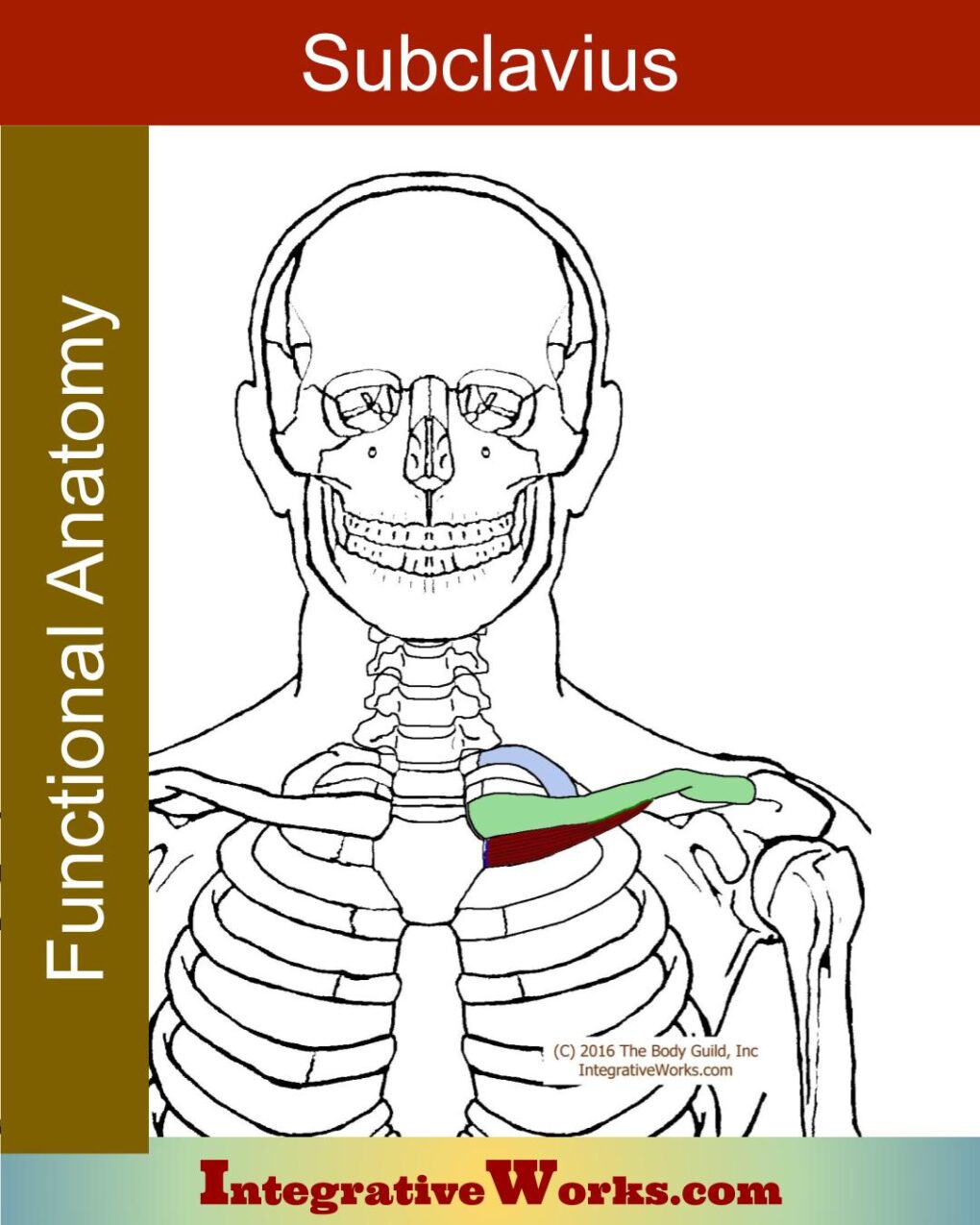
Subclavius
Subclavius is a cylindrical muscle that originates on the first rib’s costal cartilage and inserts on the underside of the medial third of the clavicle.
TOS concerns
This contributes to neurovascular pressure in several ways. First, it draws the clavicle down, trapping the neurovascular bundle between the first rib and upper belly of the serratus anterior. Also, when overdeveloped, its belly presses into the neurovascular bundle.
Subclavius trigger points refer to the upper chest, biceps, forearm, and hand. This post has more about subclavius, its trigger point patterns, self-care, massage notes, and more.
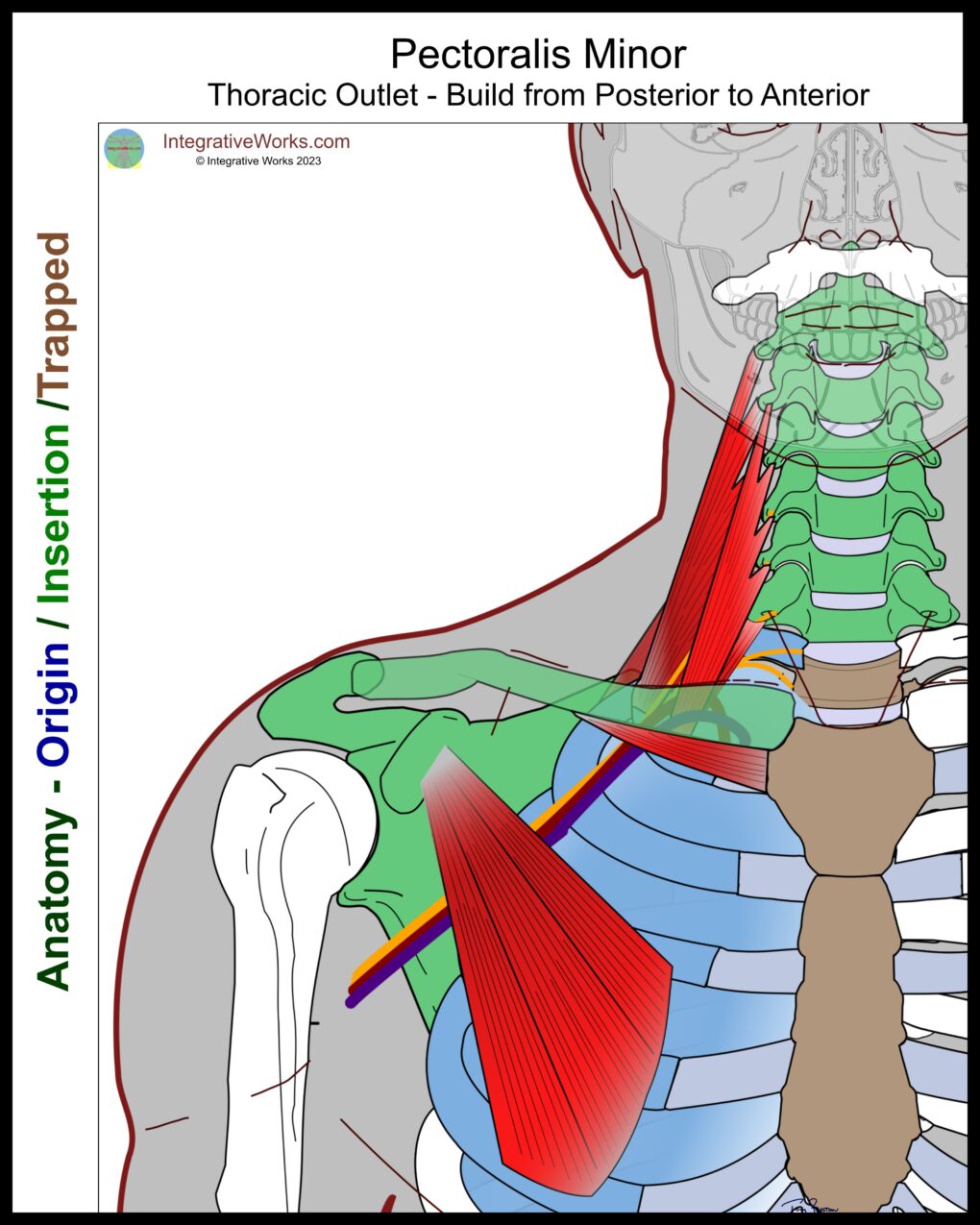
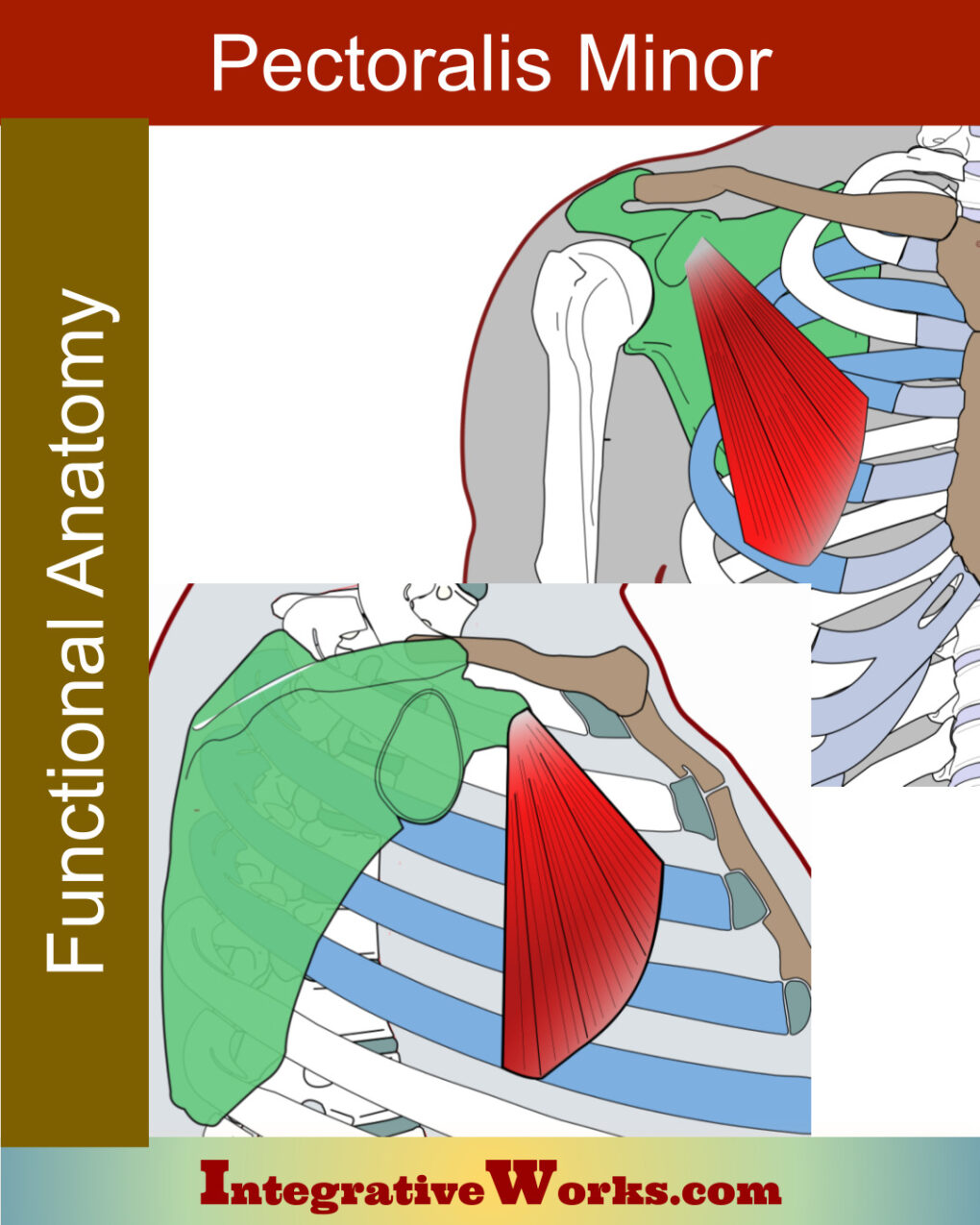
Pectoralis Minor
Most often, pectoralis minor originates on the 3rd, 4th, and 5th rib. It inserts on the medial portion of the coracoid process. More common anomalies include origins on the 2nd and 6th rib. as well as insertions that extend to the greater tubercle of the humerus.
It contributes to TOS in several ways. First, it depresses the scapula, pulling the coracoid process onto the ribs. Second, it can apply pressure on the costocoracoid membrane, which covers and protects the neurovascular bundle as it passes under the clavicle to the axilla.
The pectoralis minor trigger points refer to the chest, shoulder, forearm, and all the way down the medial border of the upper extremity. This post has more about pectoralis minor, its trigger point patterns, self-care, massage notes, and more.
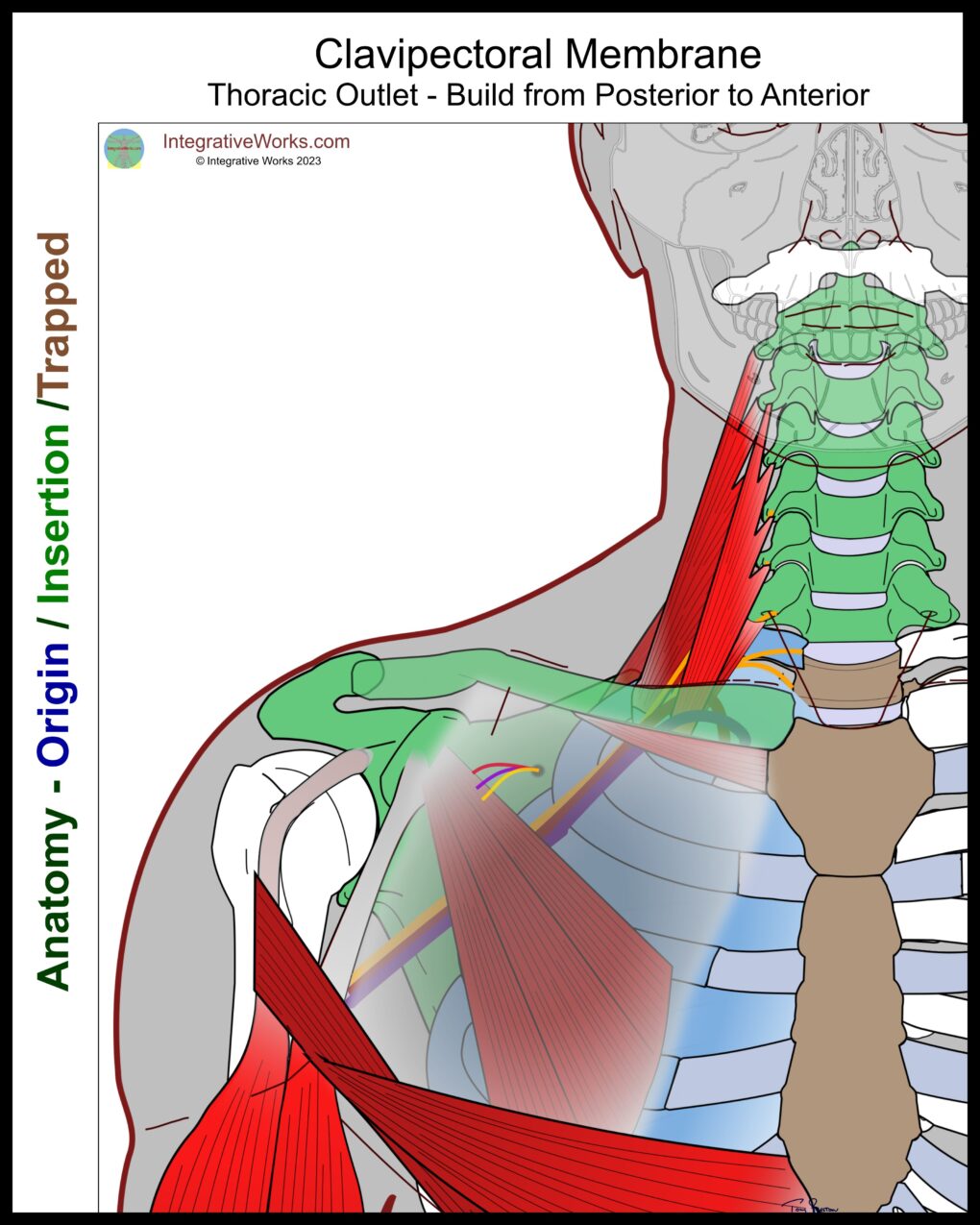
Clavipectoral Membrane
The clavipectoral membrane is a thick, dual-layered, fascial membrane that invests pectoralis and subclavius. It creates a partition that divides the area beneath the pectoralis major into superficial and deep sections. The clavipectoral membrane attaches to the clavicle, with a layer on either side of the subclavius. Those layers blend over the upper ribs and then split again as they invest the pectoralis minor.
Running along the attachments on the clavicle, the membrane is thicker. The costocoracoid ligament is a thickened portion of this membrane extending along the subclavius. Medially, it blends with the coracoclavicular ligament that secures the first rib to the clavicle. Laterally, it attaches to the coracoid ligament.
The membrane fuses into a single layer inferior to the subclavius and extends inferiorly and medially past the subclavius. It blends with the fascia over the medial aspect of the first two ribs.
The membrane continues inferiorly and splits to invest pectoralis minor. This, of course, varies with the anomalies of pectoralis minor. A number of studies examine the space between the costoclavicular membrane and the pectoralis major. Breast implants can be placed here.
I’ve included the biceps brachii in this illustration to show how this facia blends across the top of the armpit.
The suspensory ligament extends inferiorly from the lateral border of the pectoralis minor. It supports the axillary fascia, pulling the fascia up around the lateral border of the pectoralis major. This forms the depression of the armpit. The suspensory ligament attaches to the axillary fascia, which supports the lateral border of the pectoralis major.
I’ve included the costal laminae of the pectoralis major in this illustration to help show their relationships. The lower laminas of the pectoralis major twist when the arm is alongside the body. You can read more about the laminae of the pectoralis major in this post.
The thoracoacromial artery, cephalic vein, and lateral pectoral nerve lance this fascia medial to the coracoid process.
Thoracic Outlet Syndrome –
The Collection
This collection has an overview of Thoracic Outlet Syndrome as well as related posts on:
- Trigger Point Patterns of TOS muscles
- Self-Care
- Massage Notes
- Neuromuscular protocols
- Trigger Point patterns that look like TOS, but are not
Related Posts
Pain in the Torso and Arm: Signs, Pain Patterns, Self-care, Therapy Notes…
Thoracic Outlet Syndrome: Pain Patterns, Causes, Self-Care
Subclavius – Massage Therapy Notes
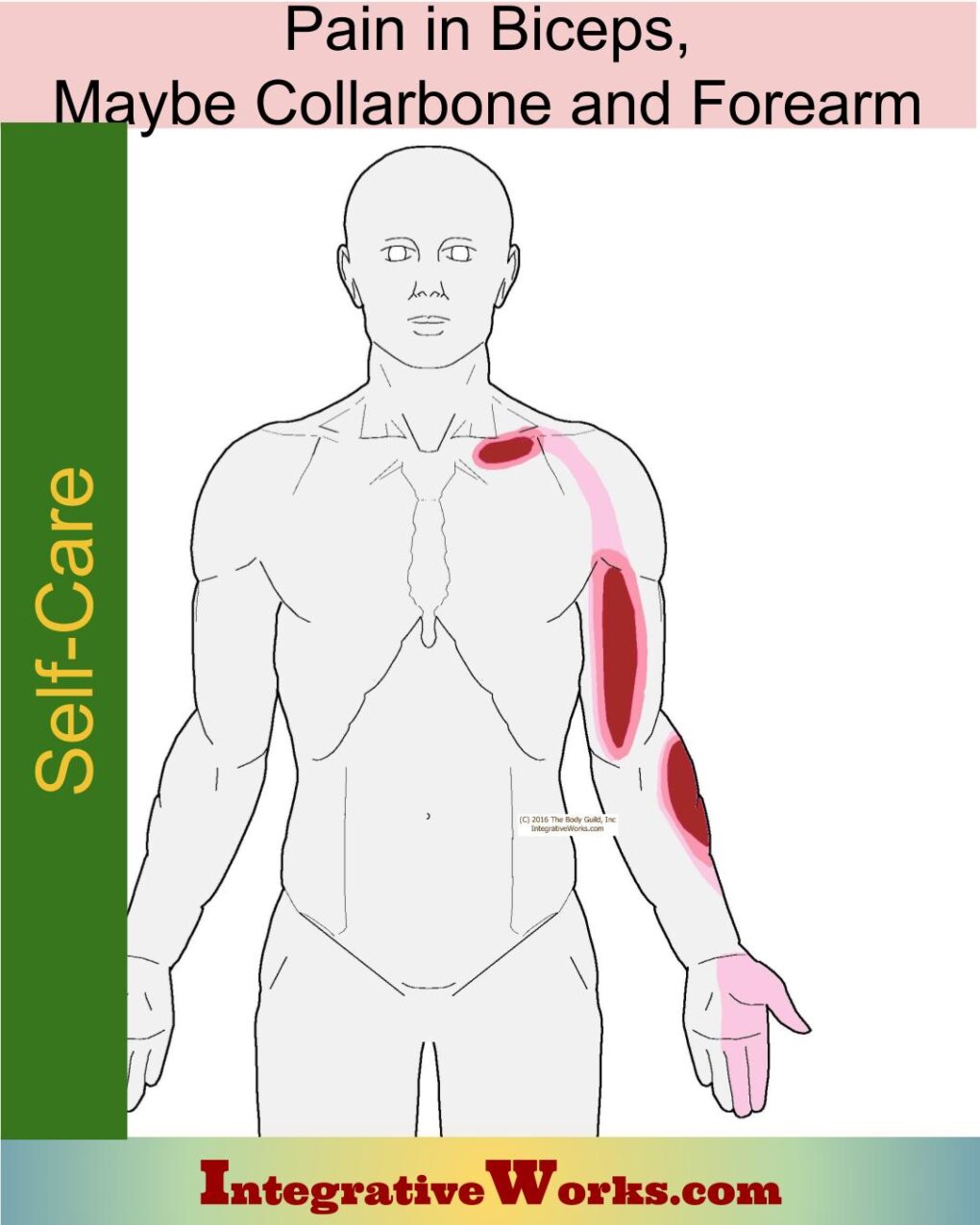
Self Care – Pain in the Biceps, Maybe Collarbone, Forearm
Self Care – Forward-Head Posture
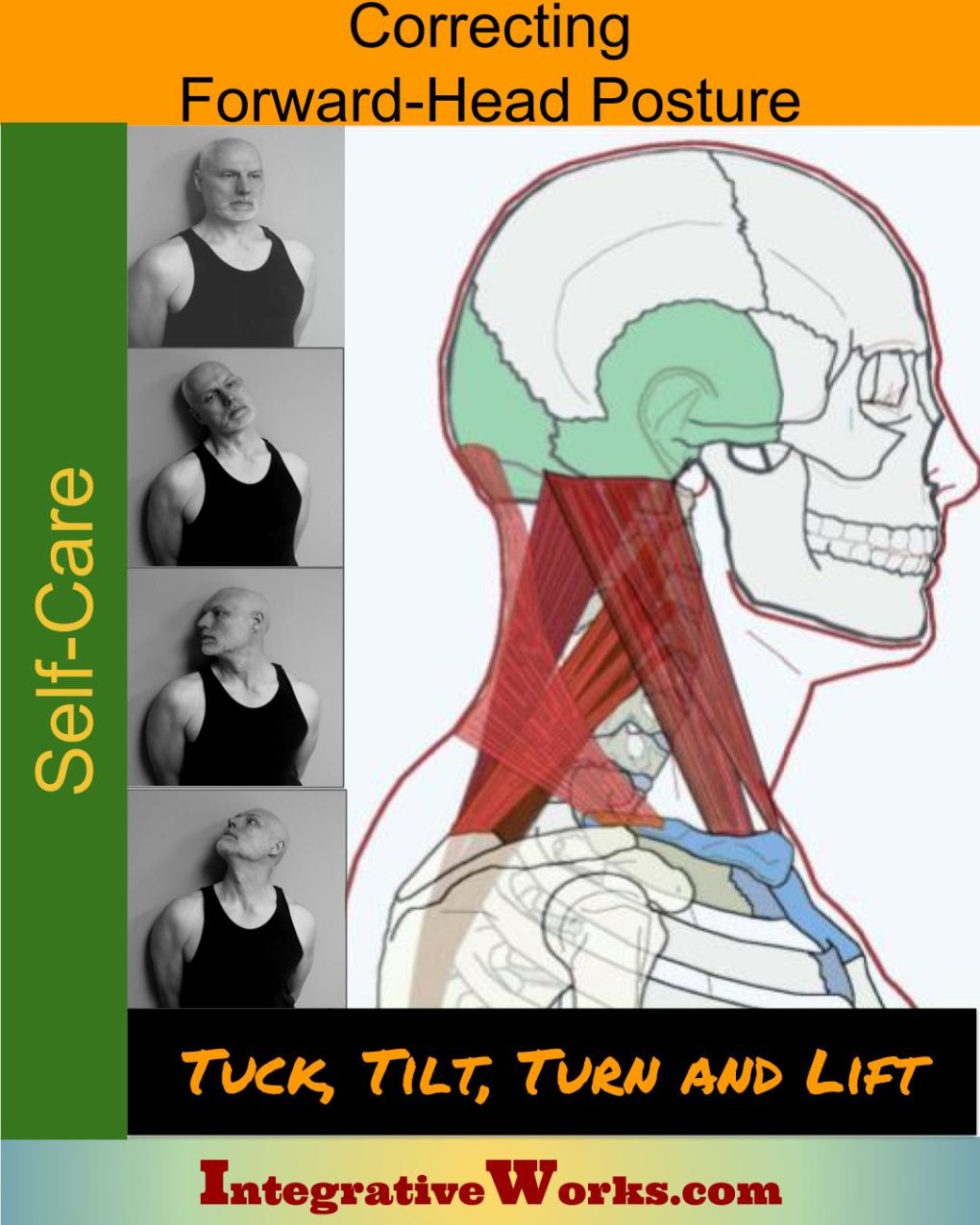
Self Care – Tuck Tilt Turn Lift to Correct Forward-Head Posture
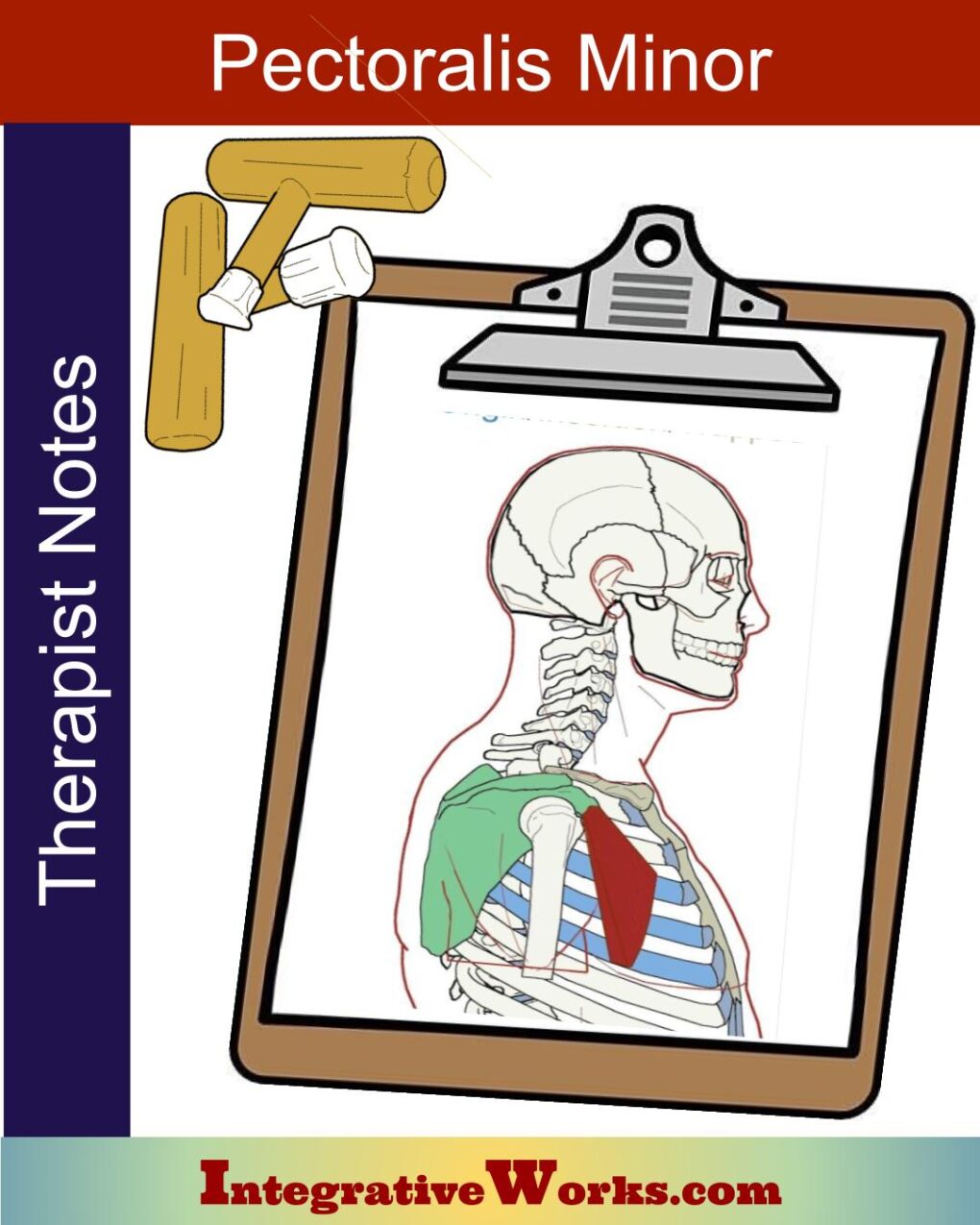
Pectoralis Minor – Massage Therapy Notes
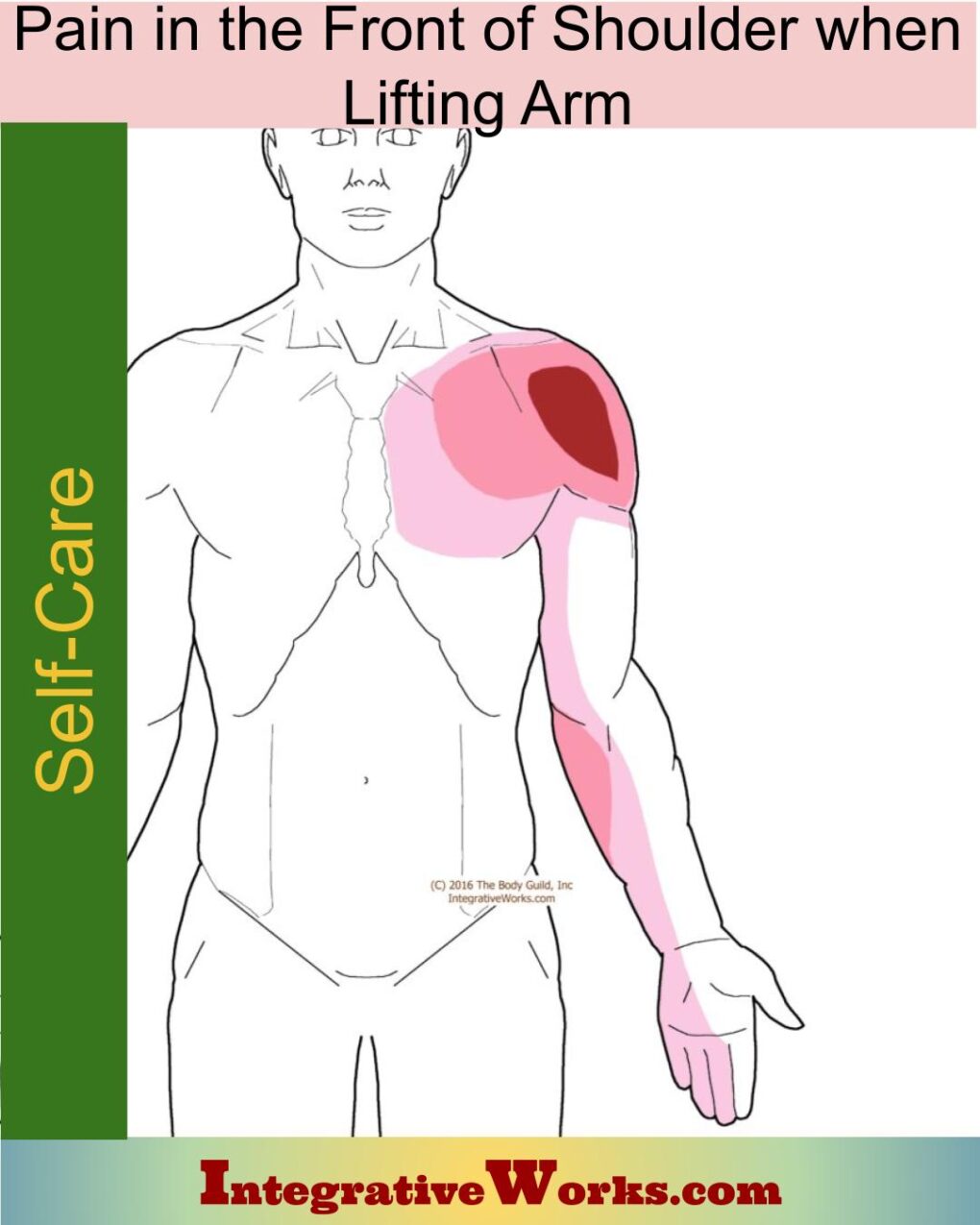
Self Care – Pain in the Front of Shoulder When Lifting Arm

Anterior Thorax (Chest) – Side Arm – Neuromuscular Massage Protocol
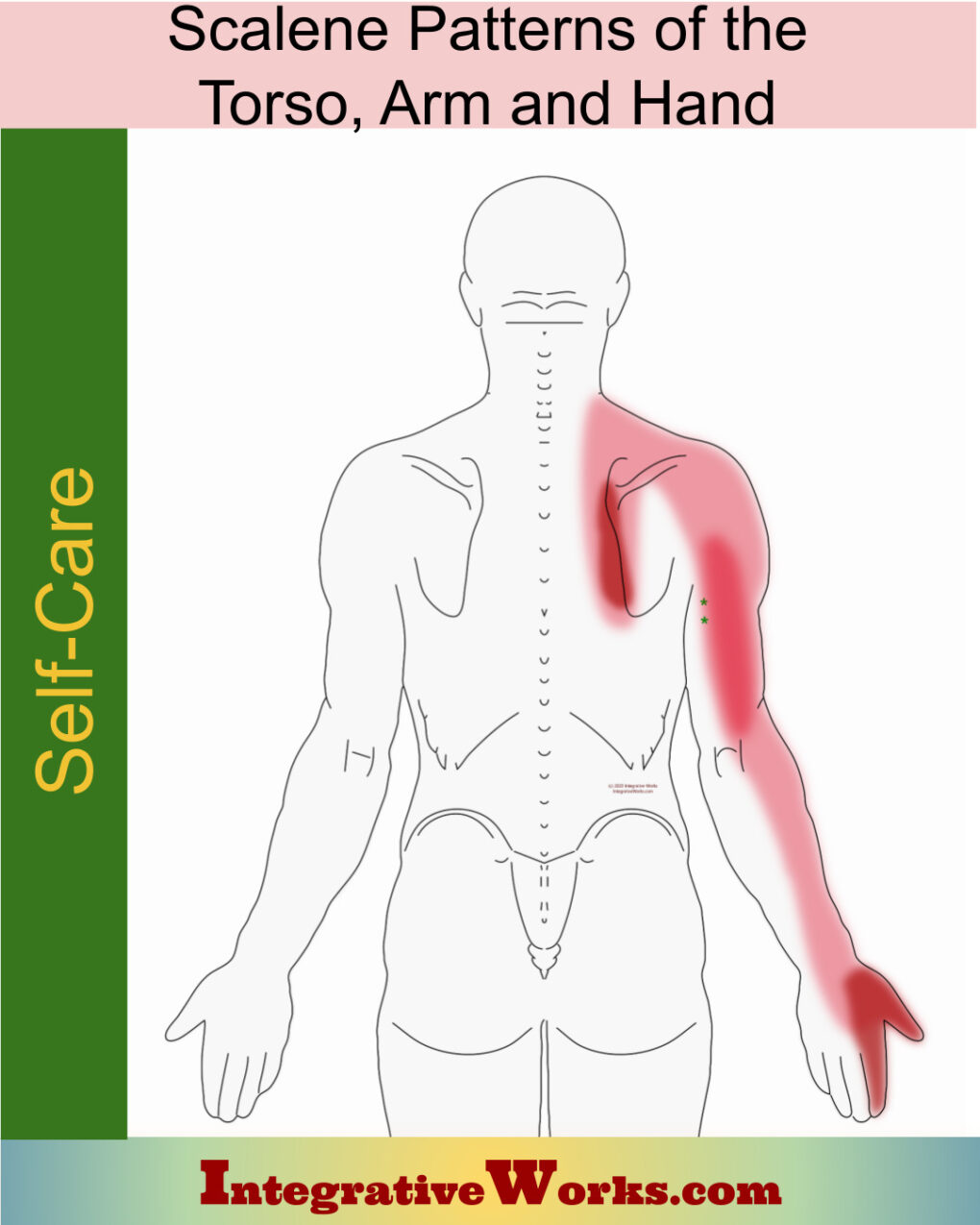
Self Care – Scalene Pain of Upper Back, Arm & Hand
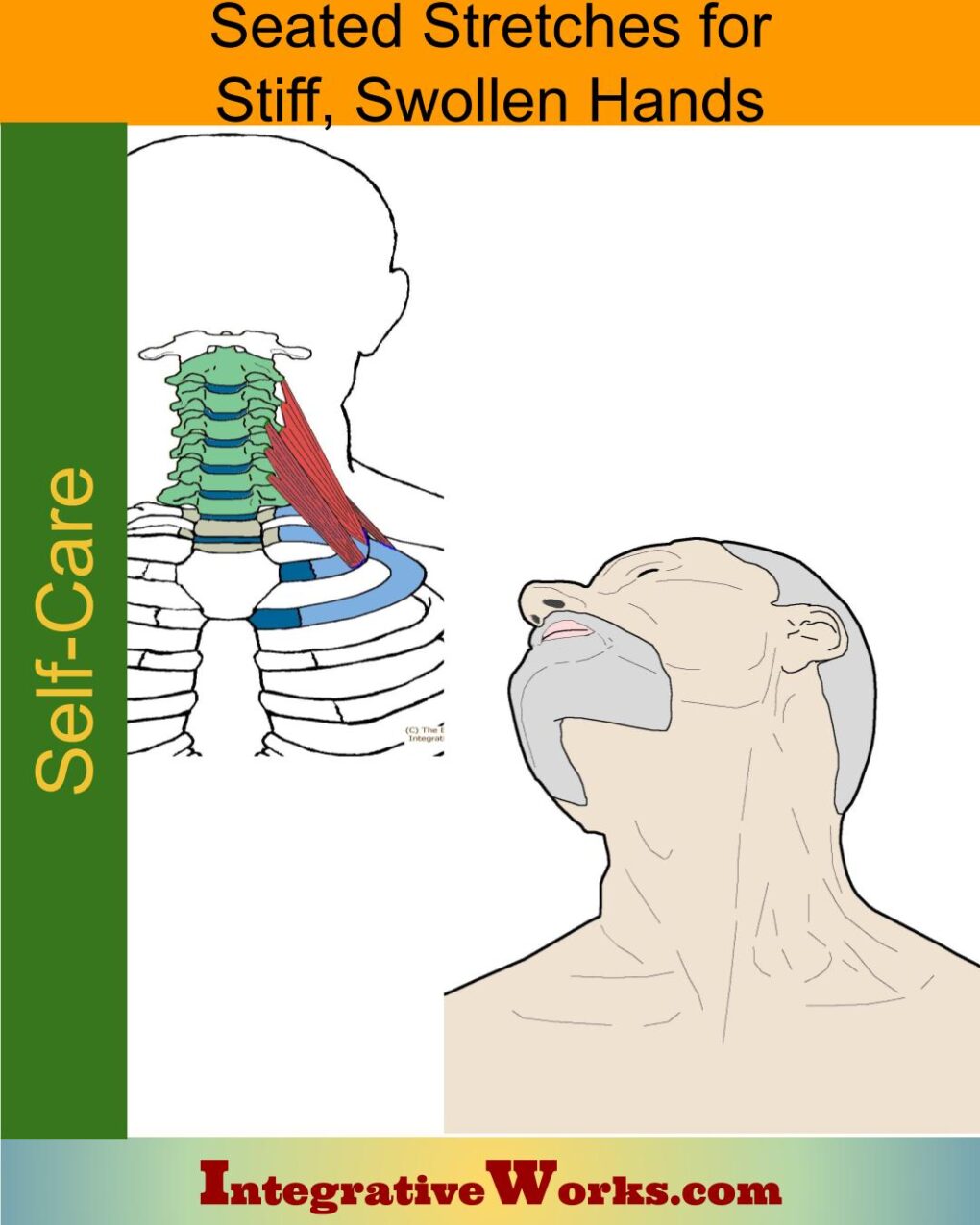
Self Care – Seated Stretches for Stiff, Swollen Hands
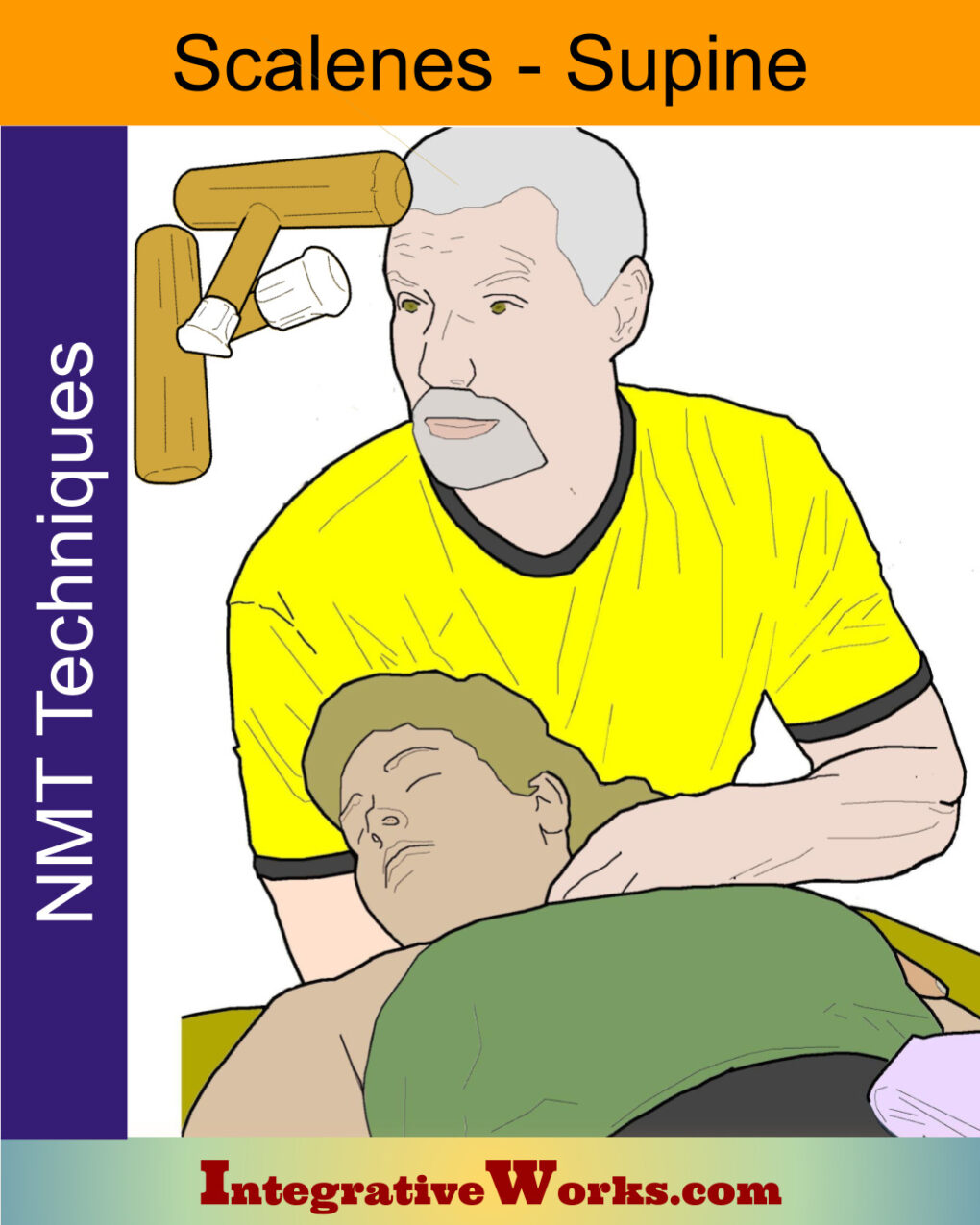
Scalenes Supine – Neuromuscular Massage Protocol
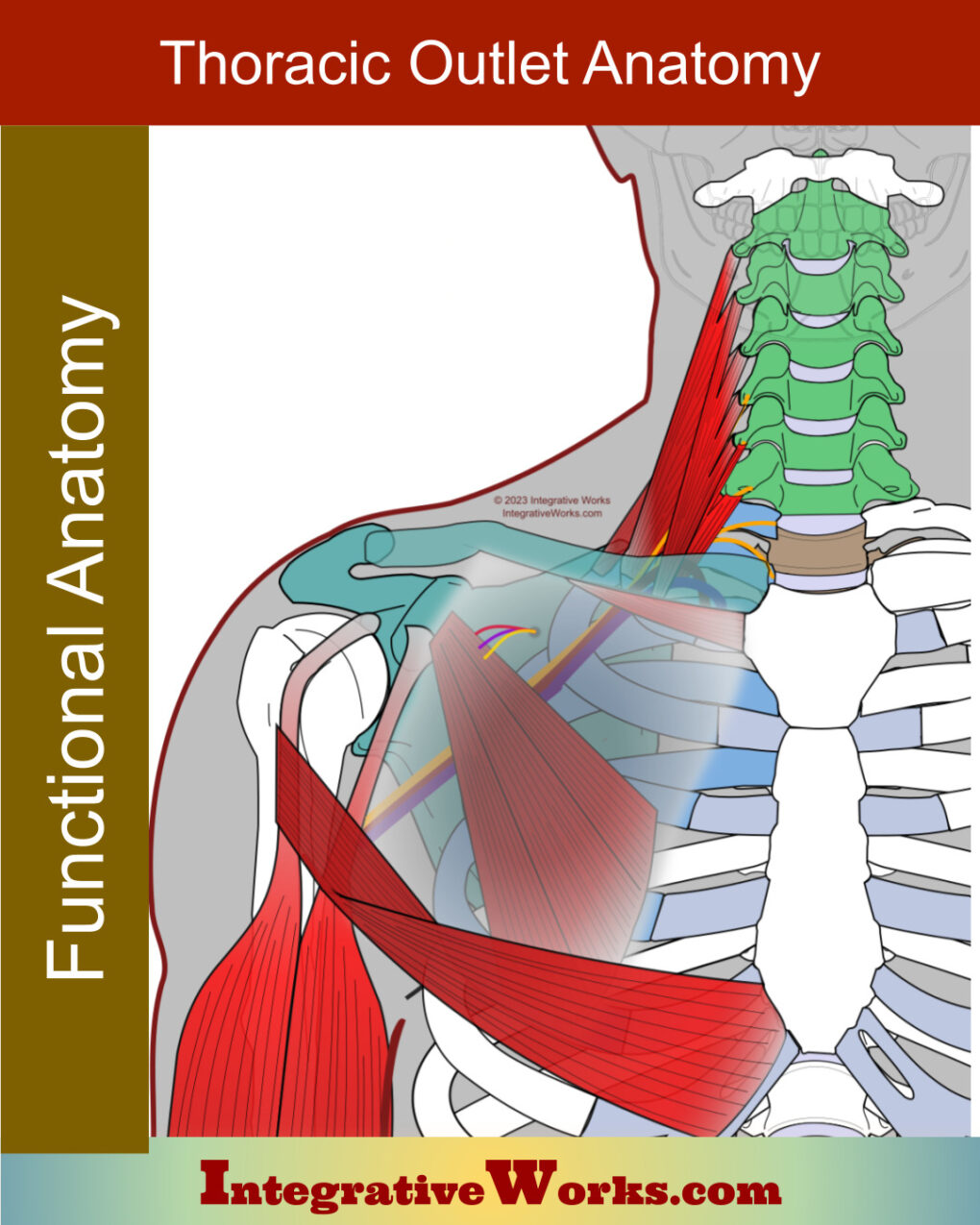
Thoracic Outlet – Functional Anatomy
Scalenes – Massage Therapy Notes
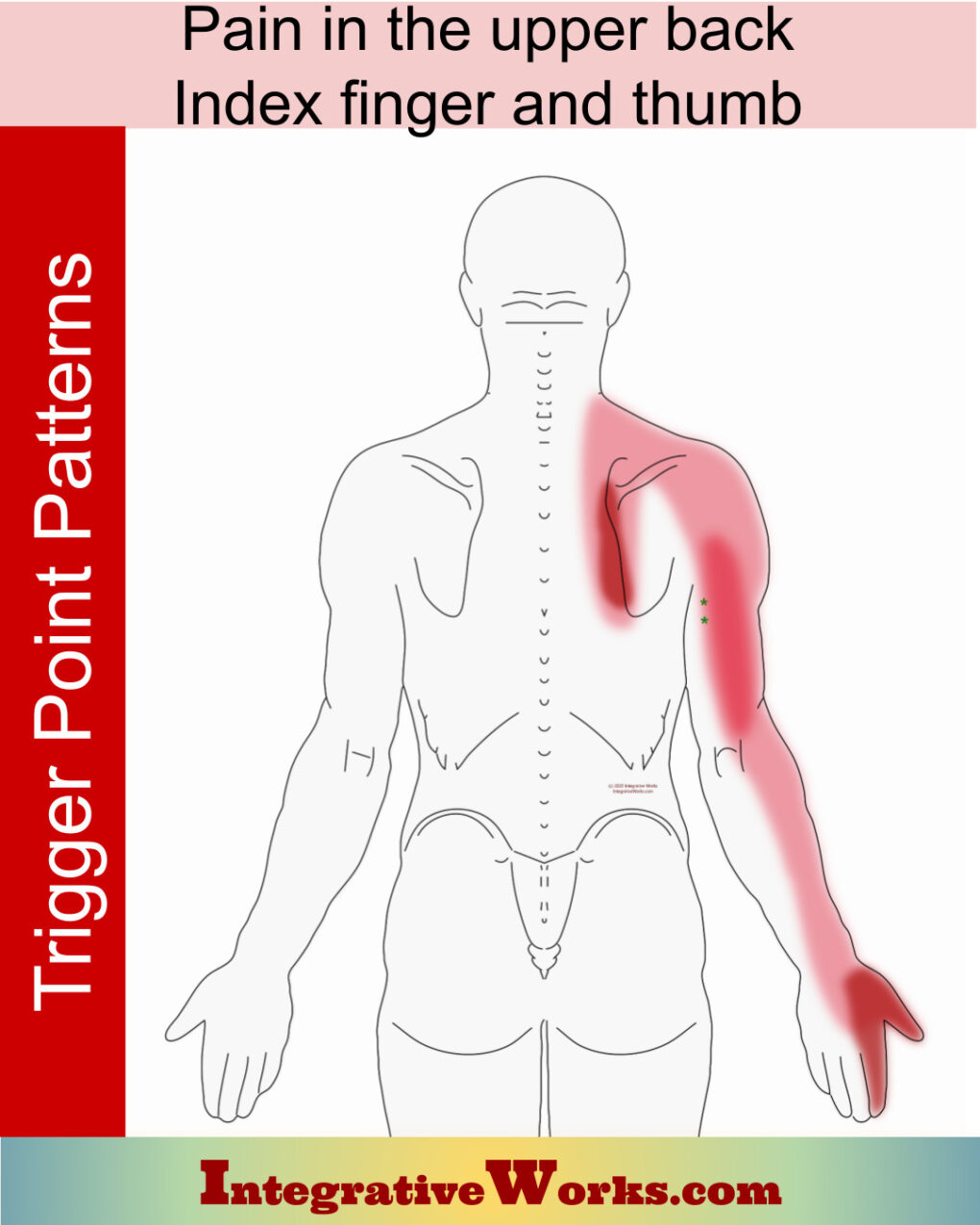
Pain in the upper back, index finger, and thumb
Scalene Muscles – Functional Anatomy
Subclavius- Functional Anatomy
Pectoralis Minor – Functional Anatomy

Pain Along the Biceps, Maybe Collar Bone & Forearm
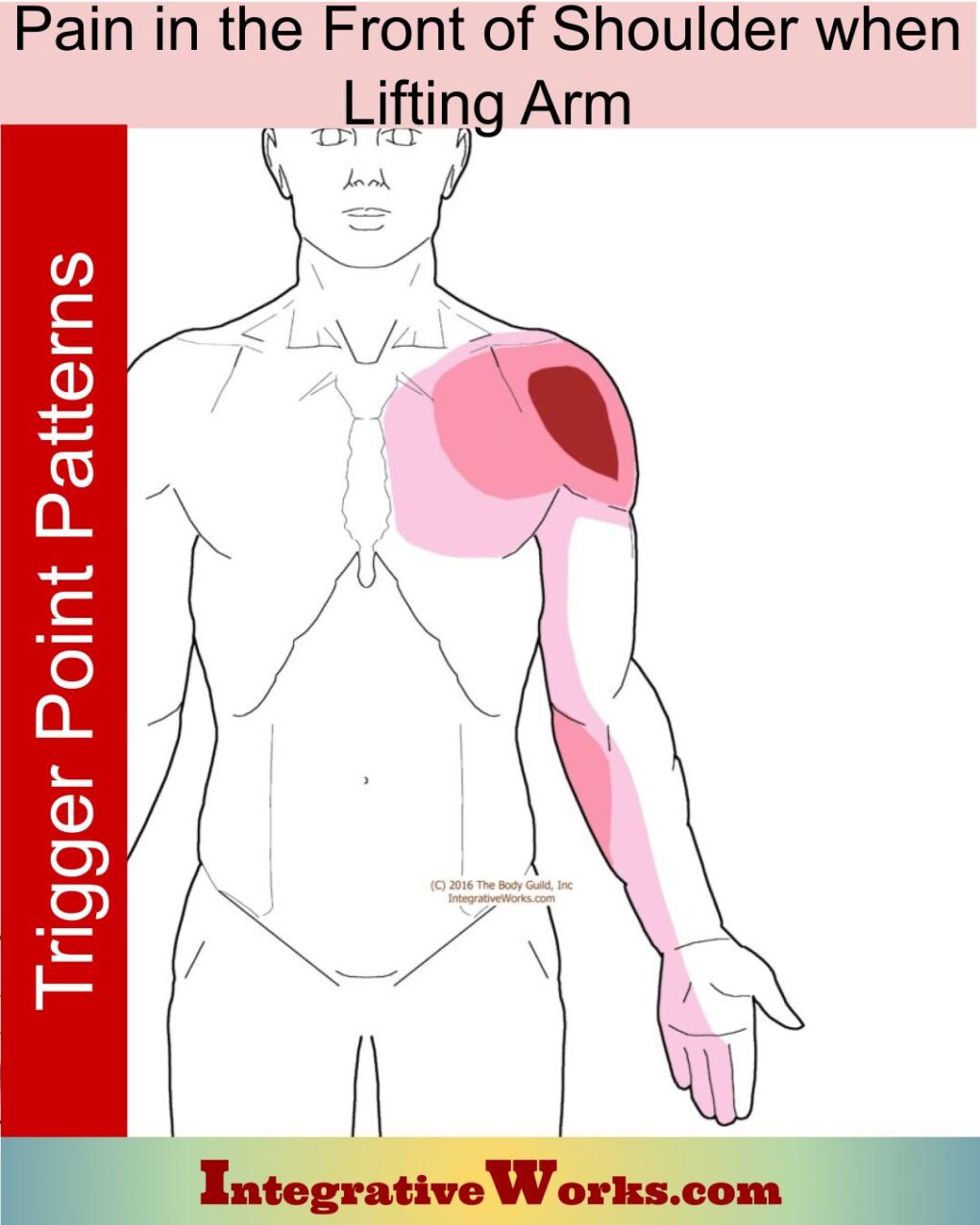
Pain in the Front of Shoulder When Lifting Arm
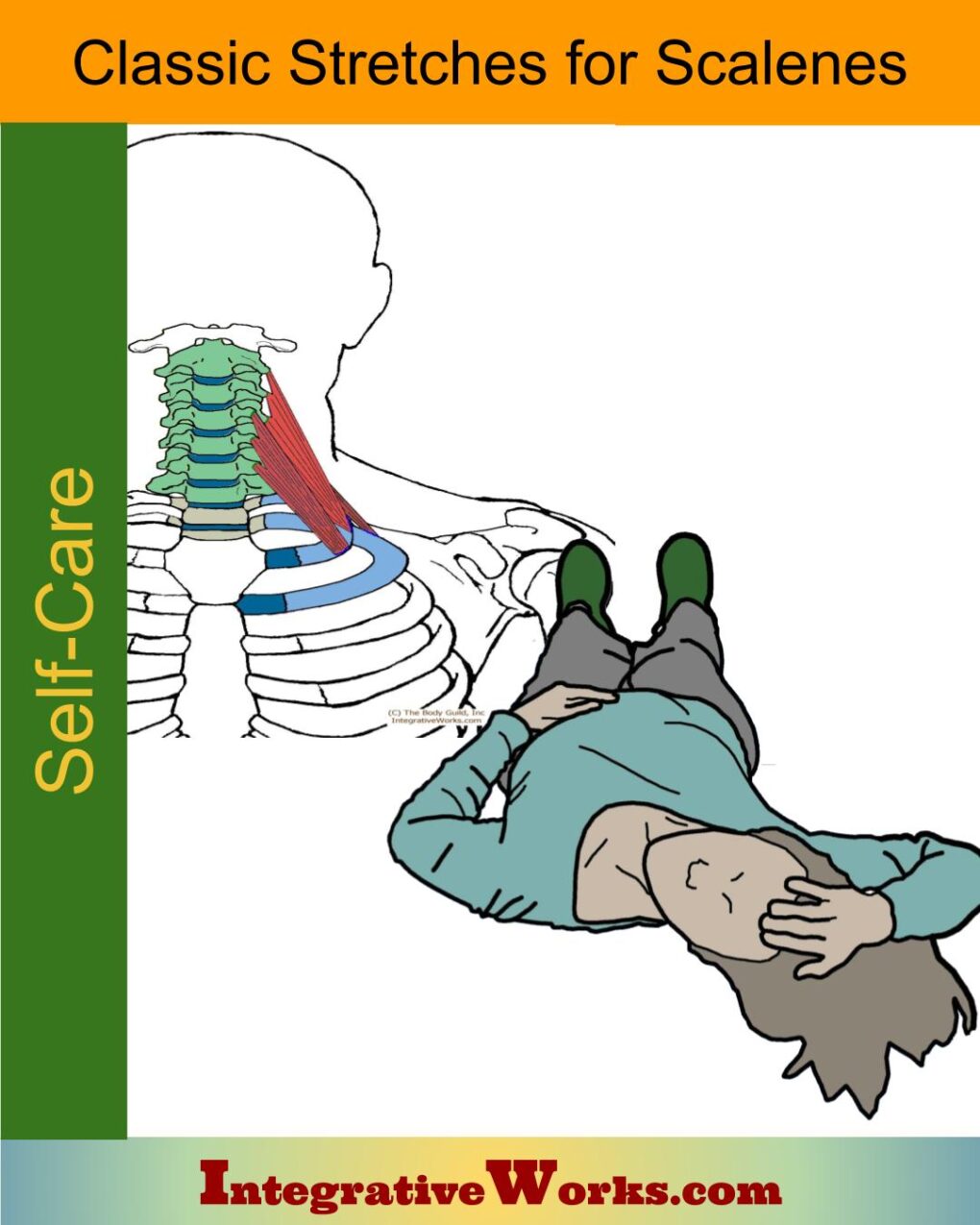
Stretching for scalene muscles
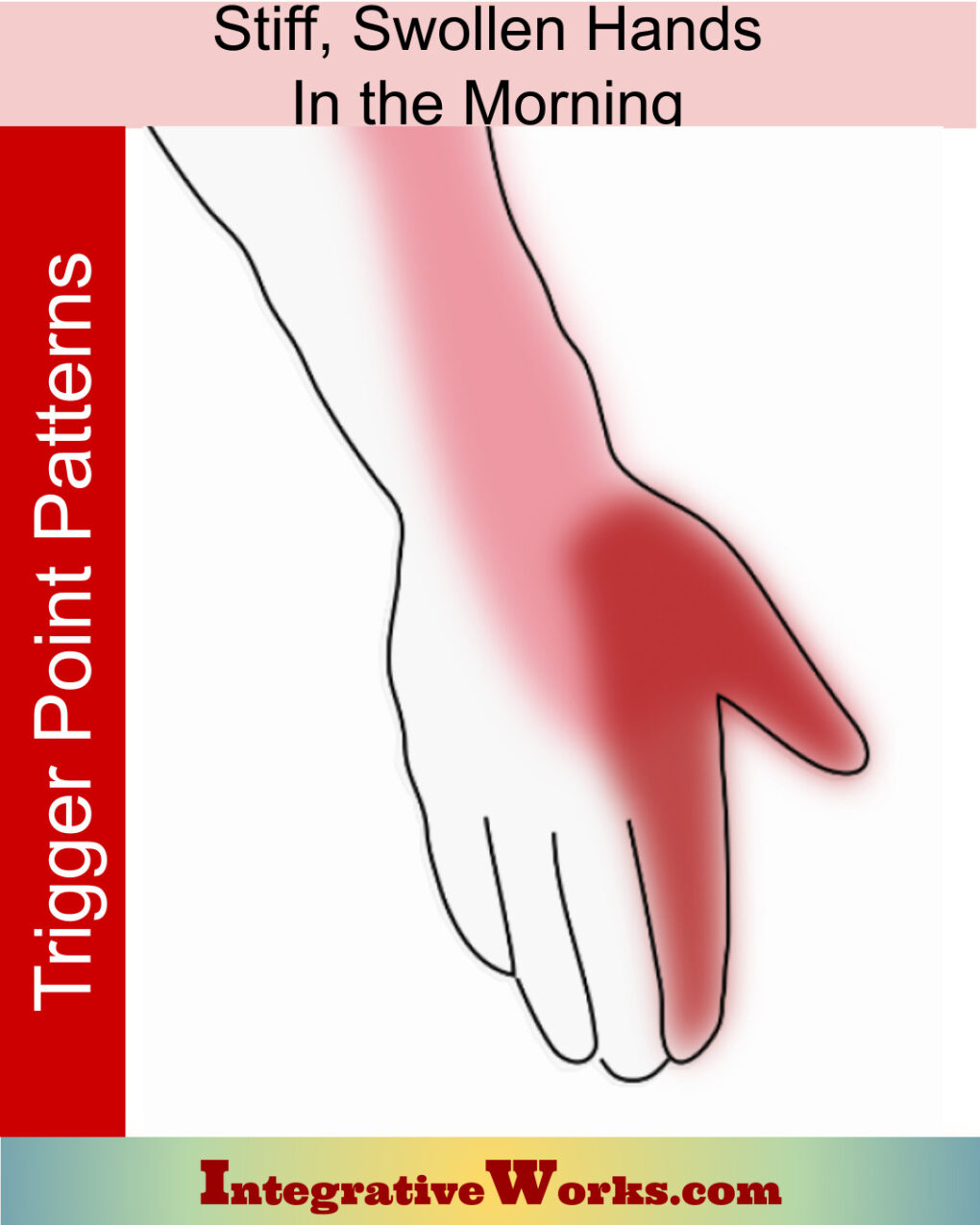
Stiff, Swollen Hands in the Morning

Self Care – Breathing exercise for upper back pain
In the end, a detailed assessment is important for efficient and effective treatment.
Support Integrative Works to
stay independent
and produce great content.
You can subscribe to our community on Patreon. You will get links to free content and access to exclusive content not seen on this site. In addition, we will be posting anatomy illustrations, treatment notes, and sections from our manuals not found on this site. Thank you so much for being so supportive.

Cranio Cradle Cup
This mug has classic, colorful illustrations of the craniosacral system and vault hold #3. It makes a great gift and conversation piece.
Tony Preston has a practice in Atlanta, Georgia, where he sees clients. He has written materials and instructed classes since the mid-90s. This includes anatomy, trigger points, cranial, and neuromuscular.
Question? Comment? Typo?
integrativeworks@gmail.com
Interested in a session with Tony?
Call 404-226-1363
Follow us on Instagram
*This site is undergoing significant changes. We are reformatting and expanding the posts to make them easier to read. The result will also be more accessible and include more patterns with better self-care. Meanwhile, there may be formatting, content presentation, and readability inconsistencies. Until we get older posts updated, please excuse our mess.