Overview
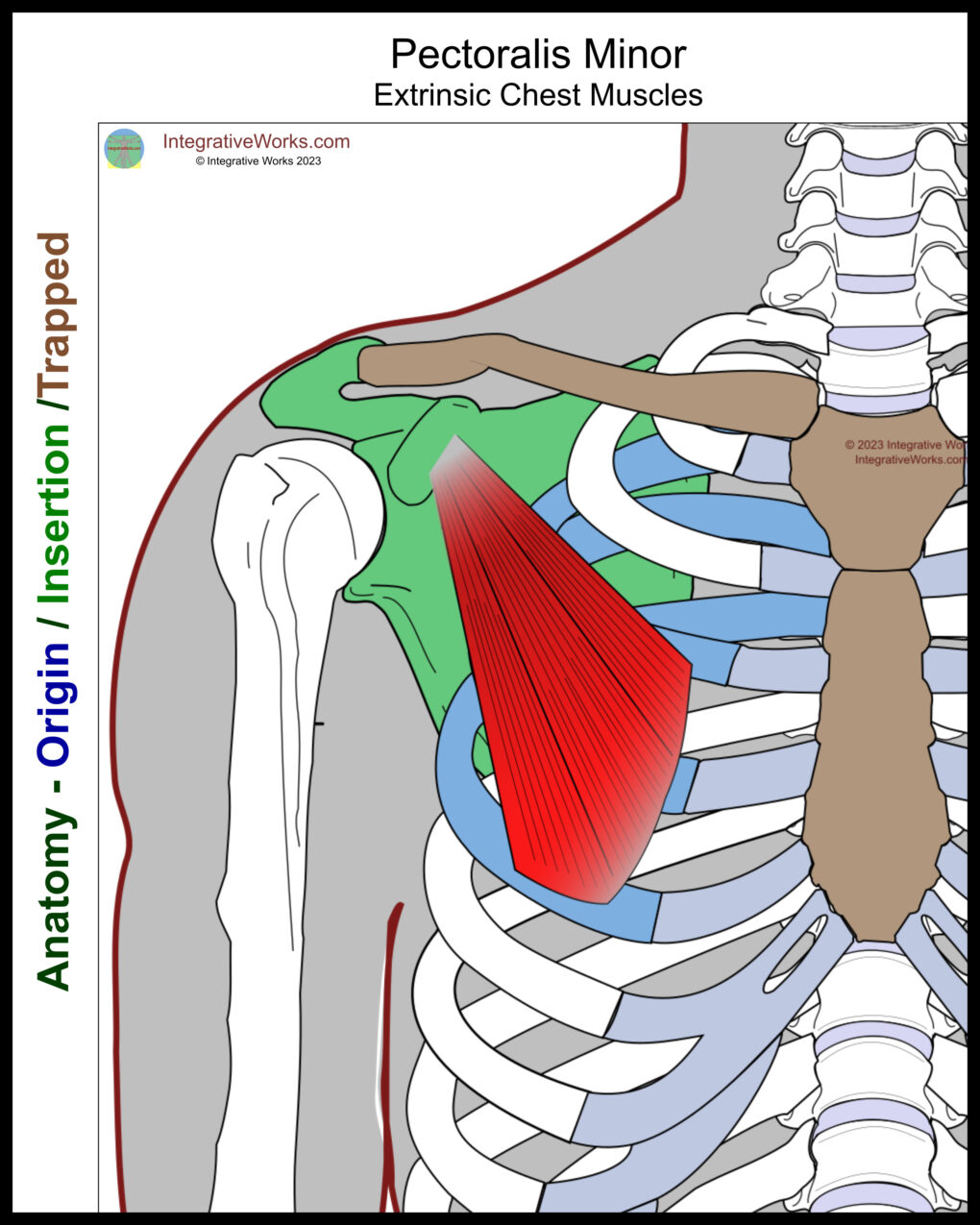
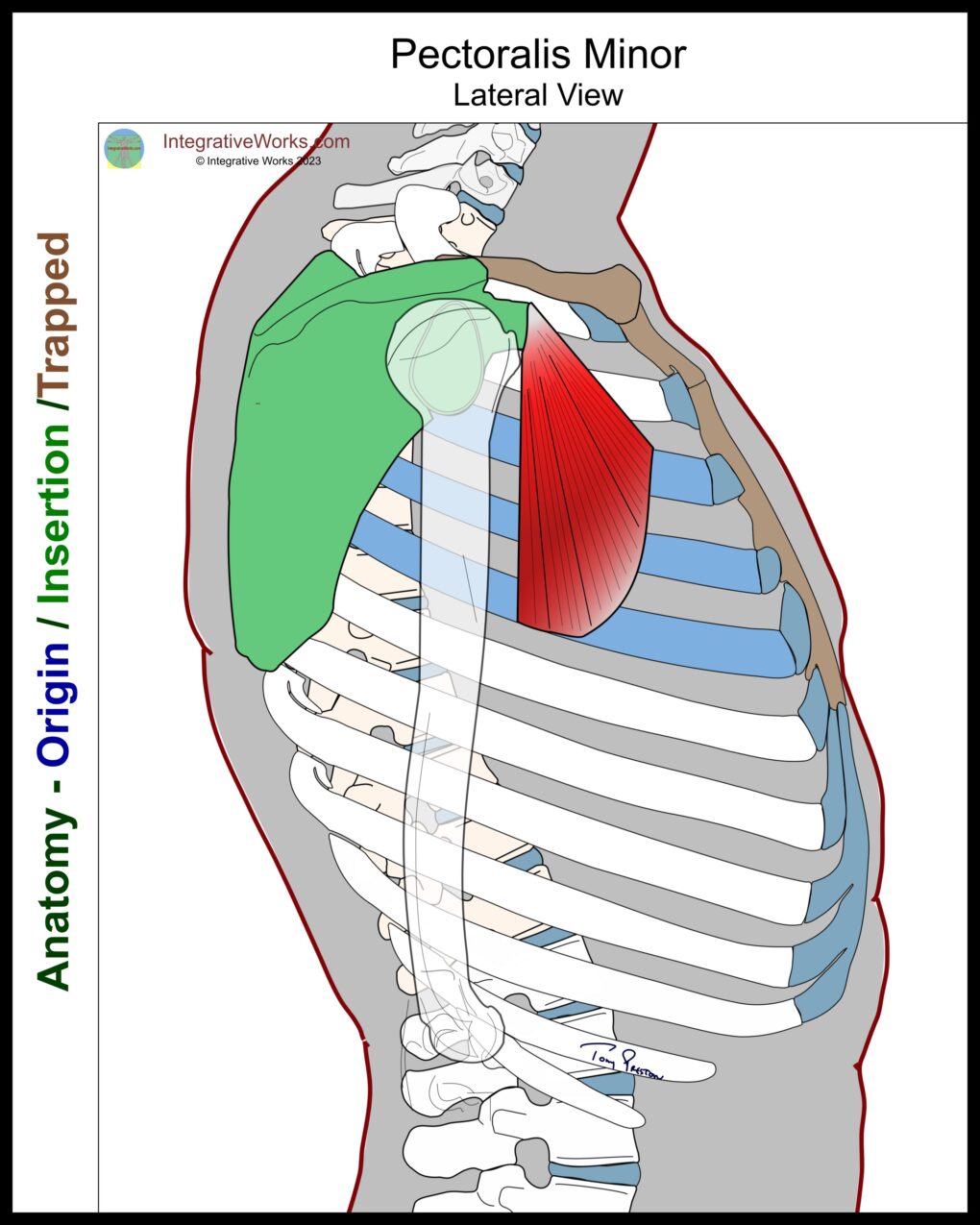
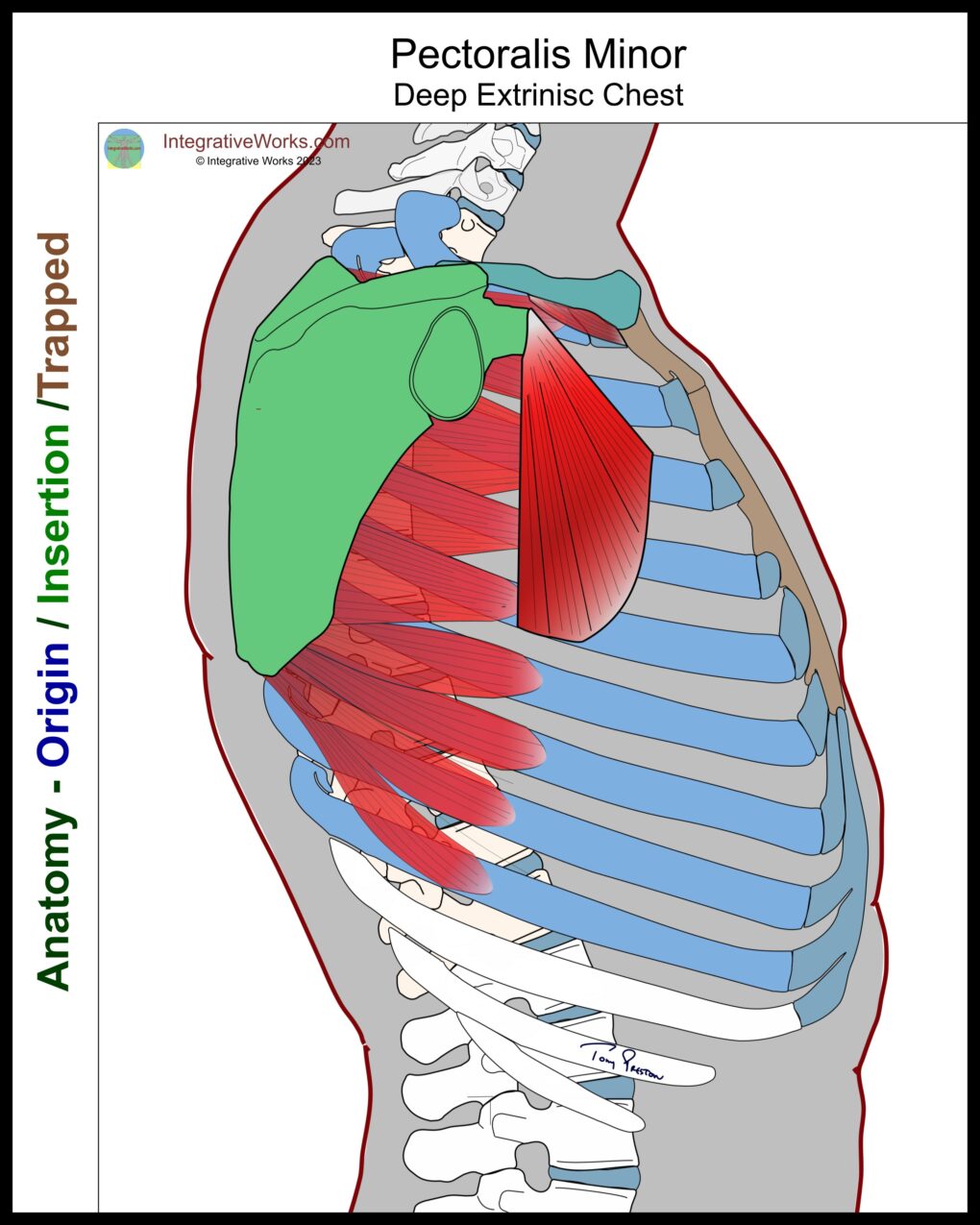
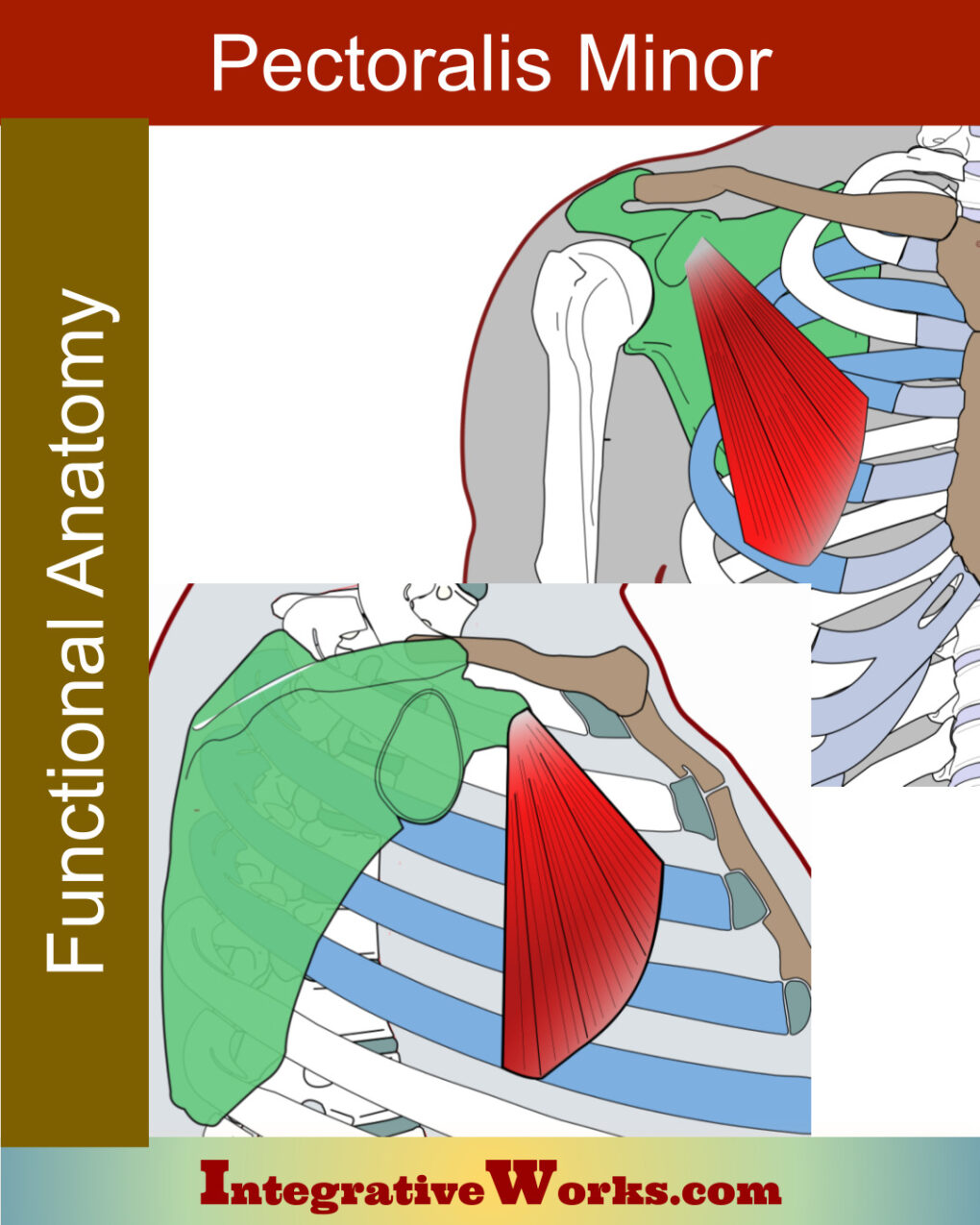
Pectoralis minor is a fan-shaped muscle in the front of the shoulder. Notably, its anatomy has frequent variations. Basically, it secures the coracoid process of the scapula to the rib cage. Superficially, the pectoralis major covers the pectoralis minor.
Overview of Pectoralis Minor Anatomy
Origin
- ribs 3-5
Insertion
- coracoid process of the scapula
Function
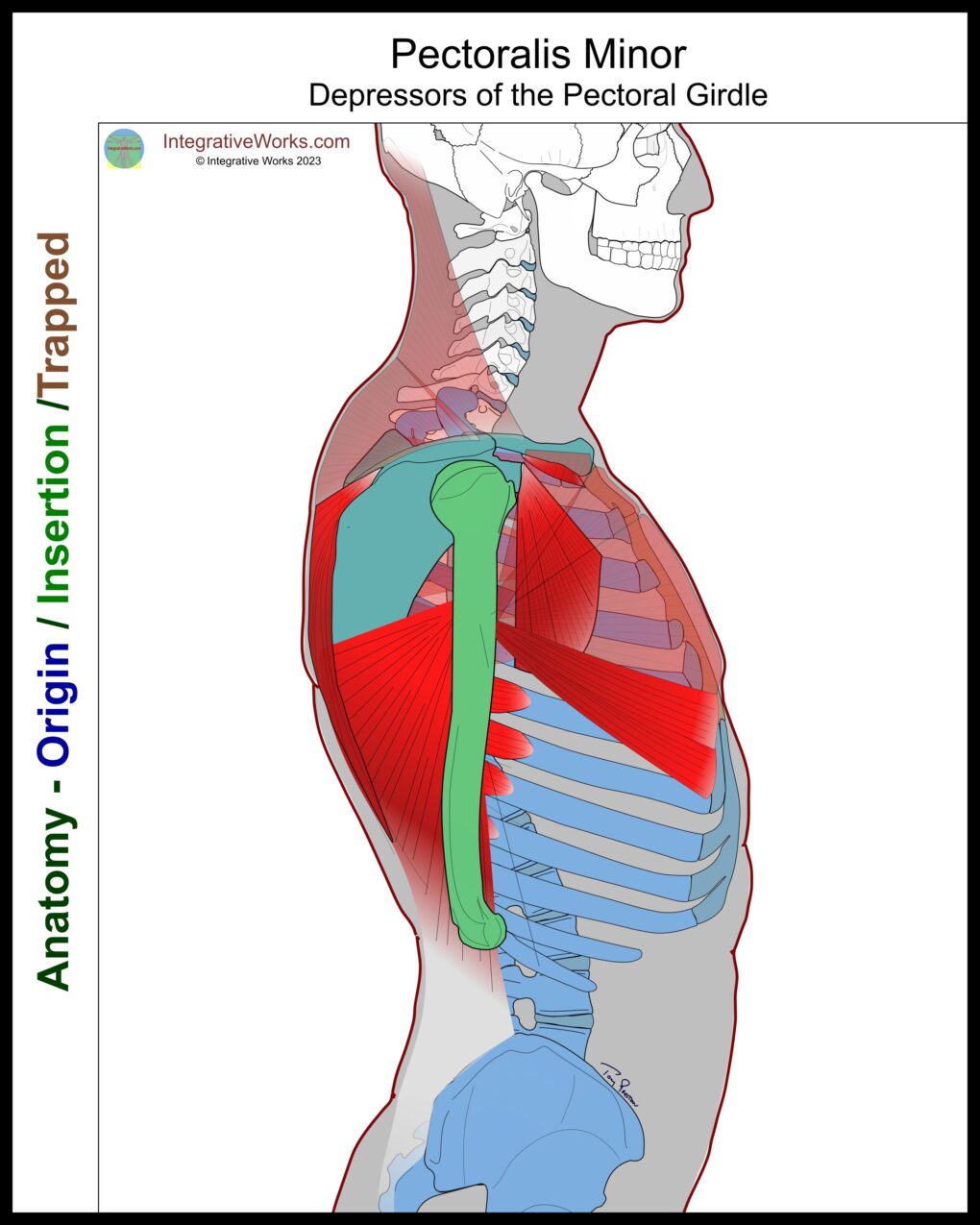
- protracts scapula
- depresses scapula
- Assists in labored breathing
Innervation
- medial pectoral nerve (C8-T1)
Anomalies are clinically significant on attachments and innervation. See the section below.
Attachment Details
The upper attachment runs along the medial aspect of the coracoid process of the scapula. This is usually a separate tendon from the coracobrachialis and biceps femoris.
The lower attachments have clinically significant variations in the number of rib attachments and their proximity to the pectoralis major. The lower attachments along the ribs are in a fan-like configuration. The underside of the attachment weaves with the intercostal aponeurosis. The superficial edge attaches to the fascia of the intercostal muscles.
Functional Considerations
The pectoralis minor has notable correlations with the vertebral bellies of the serratus anterior. The serratus anterior typically has three heads that attach along the edge of the vertebral border. (Other heads attach at the superior or inferior angle.) These three heads of the serratus anterior differ in shape from the other heads. They help elevate the scapula, whereas the lower heads depress the scapula.
When abdominal muscles stabilize the ribs, the pectoralis minor protracts and depresses the scapula. It stabilizes the pectoral girdle during downward movements like chopping wood or walking with a crutch. The pectoralis major, subclavius, and latissimus dorsi synergize to depress the pectoral girdle.
When the upper back muscles stabilize the pectoral girdle, the pectoralis minor lifts the ribs for inhalation, especially during labored breathing. It synergizes with scalenes, serratus posterior superior, and serratus anterior to lift the upper ribs and increase lung capacity. You can read more about that in the collection on Pain with Breathing.
Anomalies, Etc.
Noted anomalies include a common tendon with the biceps and coracobrachialis. One study showed that the upper attachment extends to the glenohumeral capsule in about 23% of cases.
This other study of 40 cadavers claims that the most common variation is a clavicular head.
The space between the pectoralis minor and major attachments has been studied for breast implants. Some implants attach under the pectoralis major. Unexpectedly, 49 women and 53 men participated in this study. The distance between attachments varies greatly. Notably, 24% were less than 1cm, 41% were between 1 and 3cm, and 70% were over 3cm.
Frequently, a head attaches to the second rib. In fact, it is frequent enough that some sites and studies list ribs 2-5 as the attachment. This study mentions that cadavers showed attachments to the fourth rib in 100% of cases. But, attachments to the 5th rib occurred 78% of the time and the 6th rib 3% of the time.
Most texts name the medial pectoral nerve for innervation. The lateral pectoral nerve weaves into the brachial plexus and is involved, as well as making the nerve roots C5-T1.
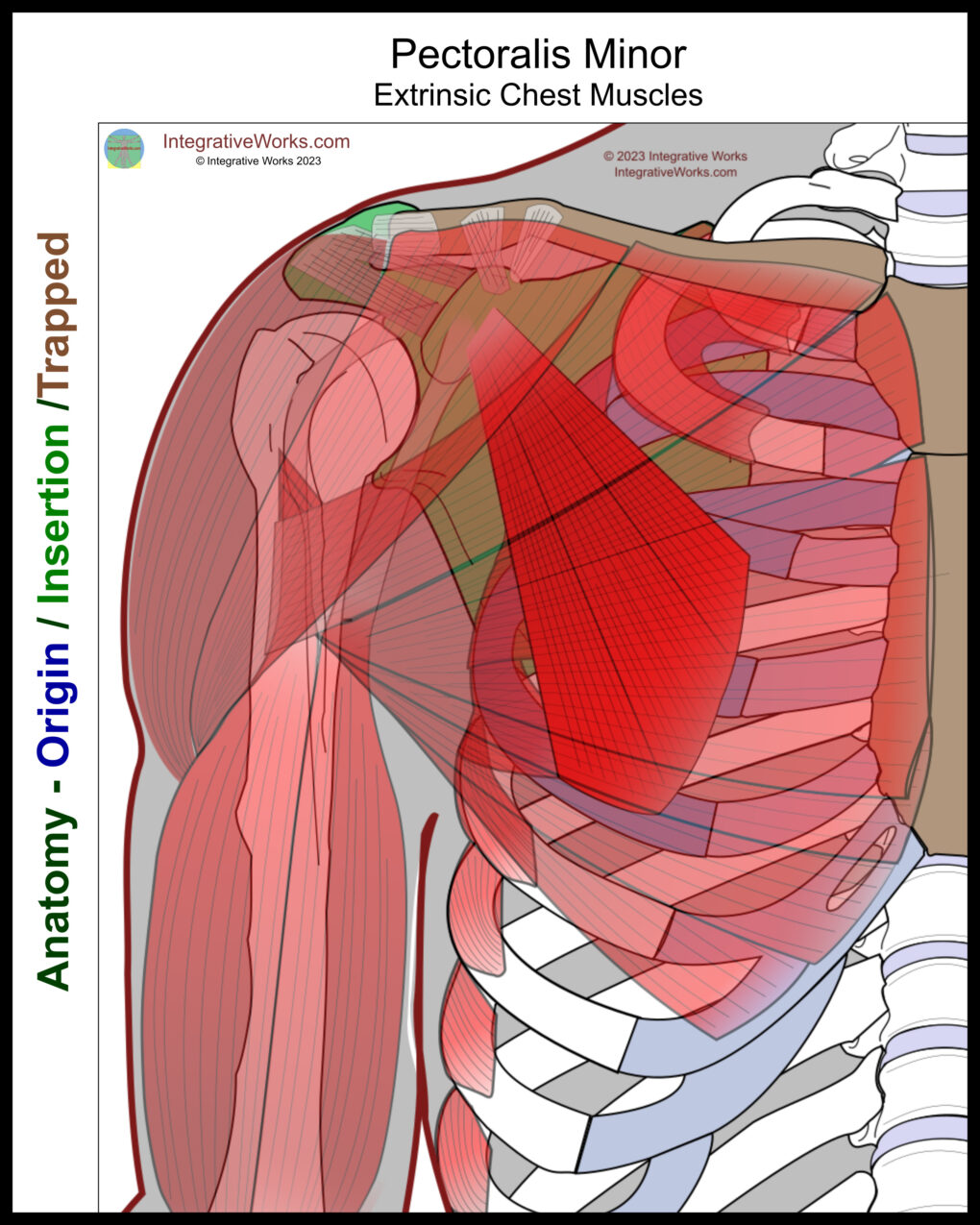
Deep Extrinsic Chest Muscles
The deep extrinsic chest muscles lie under the pectoralis major. They attach to the ribs and protract the pectoral girdle.
They consist of:
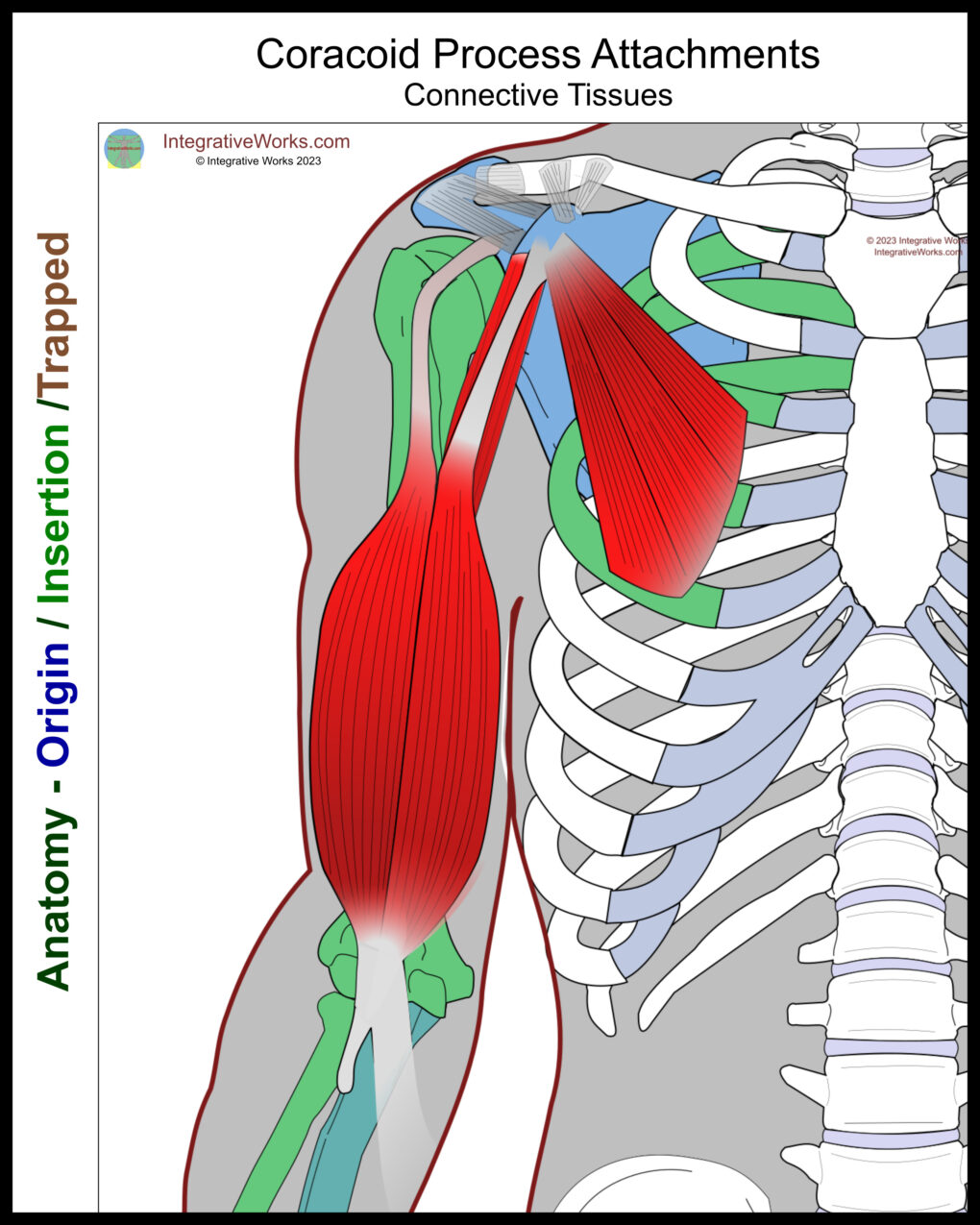
Coracoid Process Attachments
This perspective shows the coracoid process as an origin point. Consequently, the scapula is a platform that lifts the upper extremity and chest. The extrinsic back muscles would need to stabilize the pectoral girdle.
Conversely, it could be the insertion when those same muscles are used to mobilize the scapula. For example, when swinging from a limb or swimming.
They consist of:
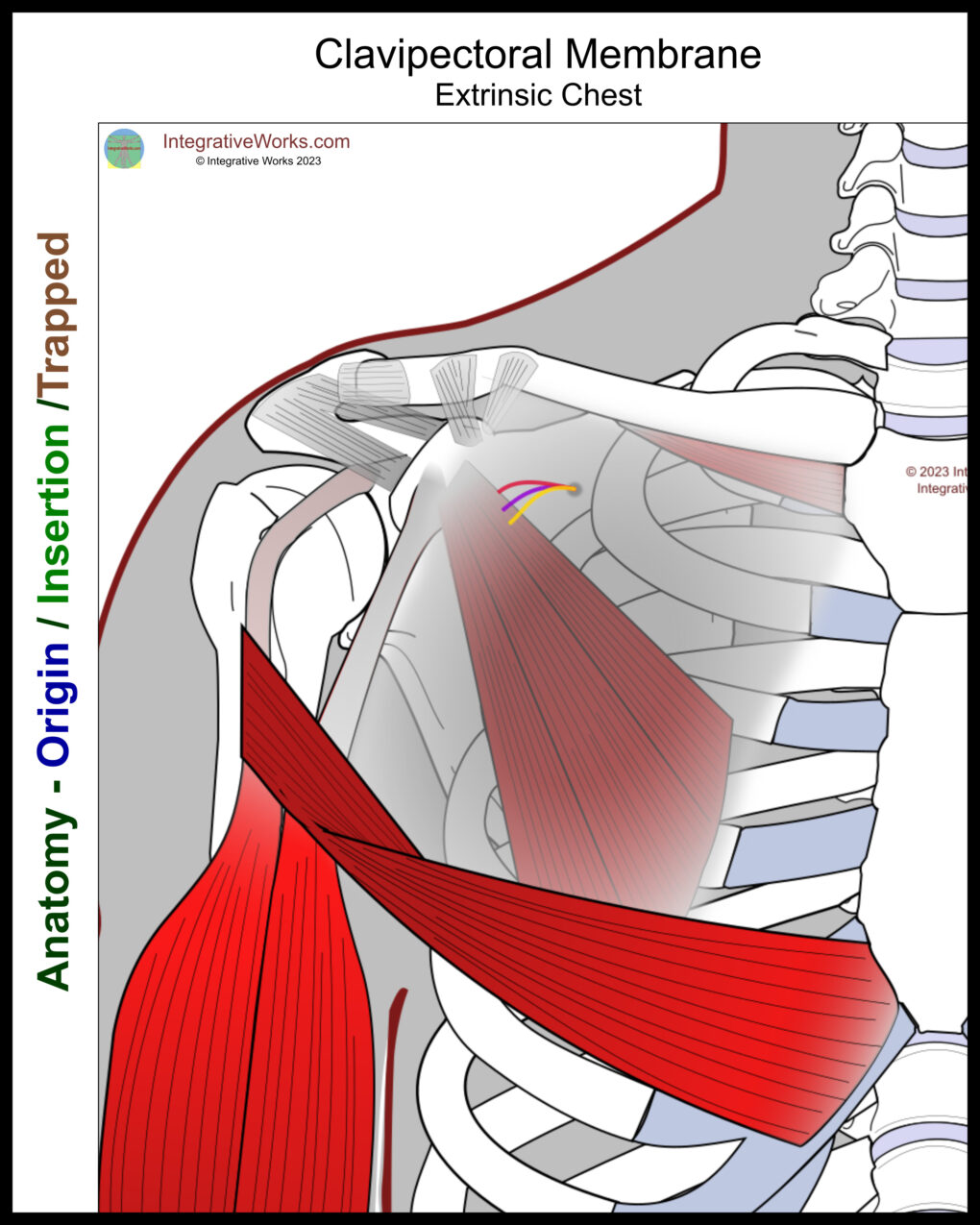
Clavipectoral Membrane
The clavipectoral membrane invests the pectoralis minor and subclavius. This fascial structure forms a sheet extending across the upper chest. This membrane ties together the upper ribs, subclavius, pectoralis minor, clavicle, and coracoid process. The upper portion is referred to as the costocoracoid membrane.
This membrane anchors to the coracoid process of the scapula. Also, it attaches superiorly to the clavicle, investing the subclavius. Next, the medial border extends along the ribs between the pectoralis minor and major. Then, the inferior border attaches to the pectoralis major. Finally, the lateral border extends along the biceps tendon, connecting it to the coracoid process.
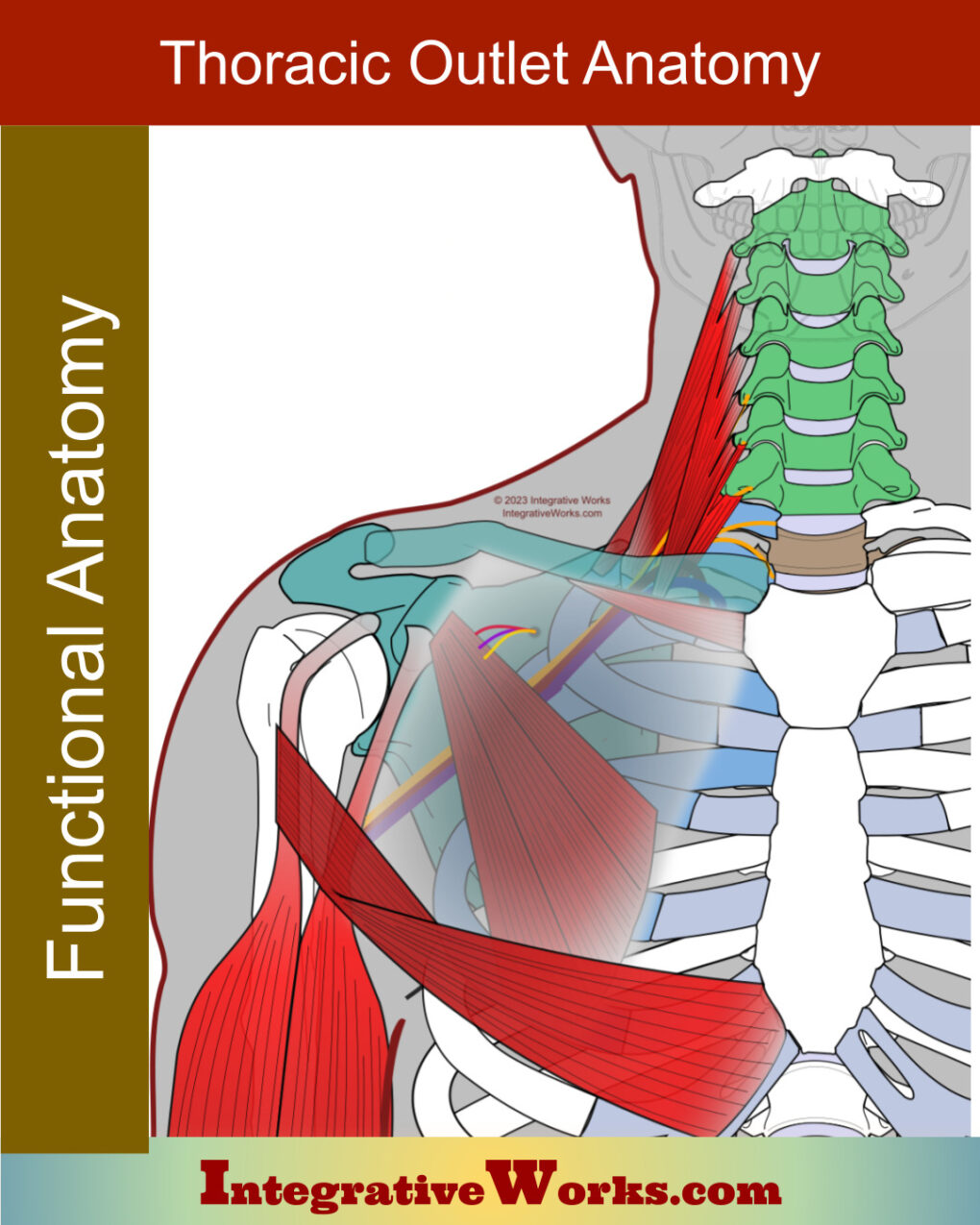
This membrane also covers the neurovascular bundle that feeds the upper extremity, making it an important part of Thoracic Outlet structures. You can read more about these structures in this post about the Anatomy of Thoracic Outlet Syndrome.
Related Posts

Anterior Thorax (Chest) – Side Arm – Neuromuscular Massage Protocol
Anterior Thorax Supine – Neuromuscular Massage Protocol
Assessment of Pain in Yoga
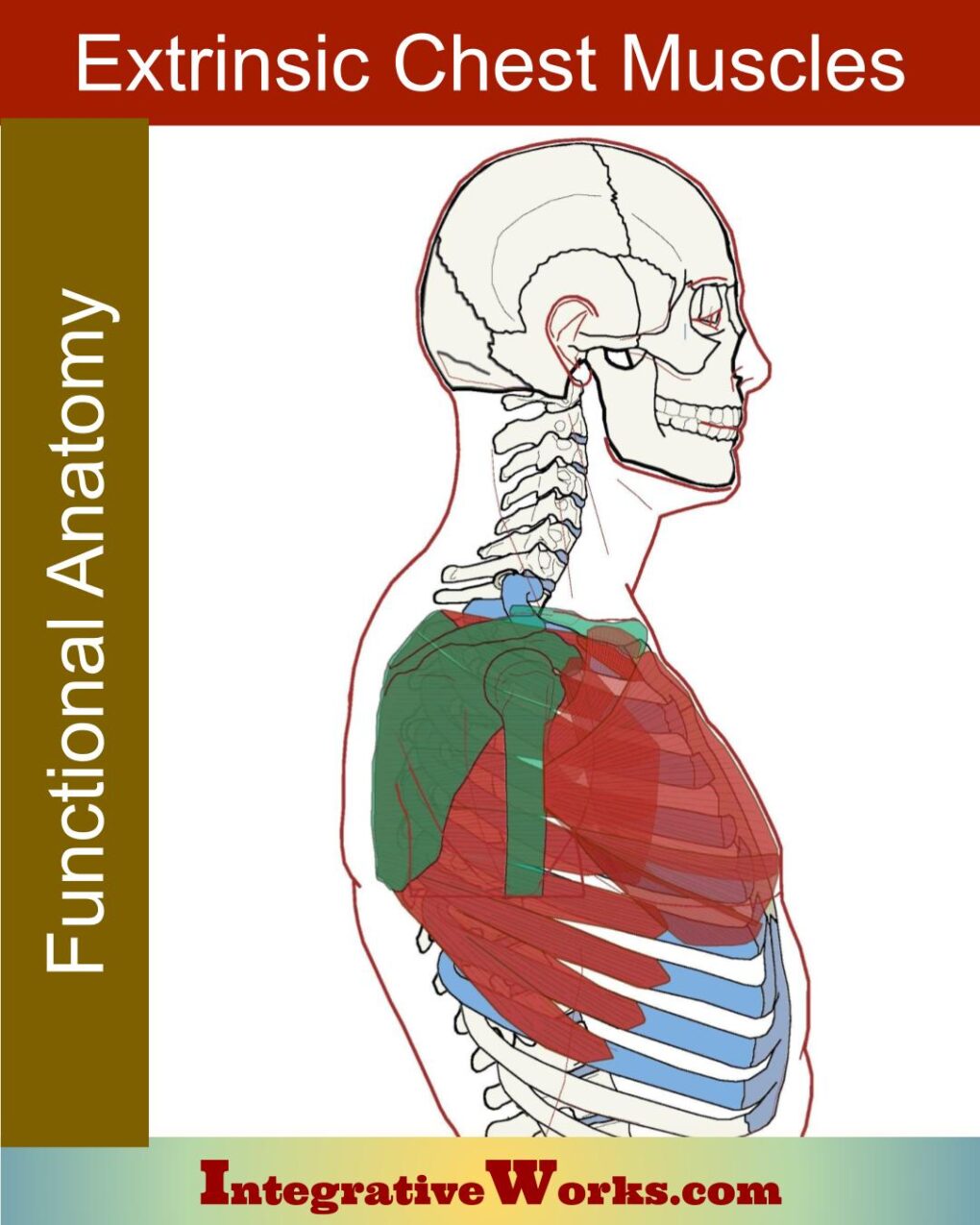
Extrinsic Chest Muscles – Functional Anatomy
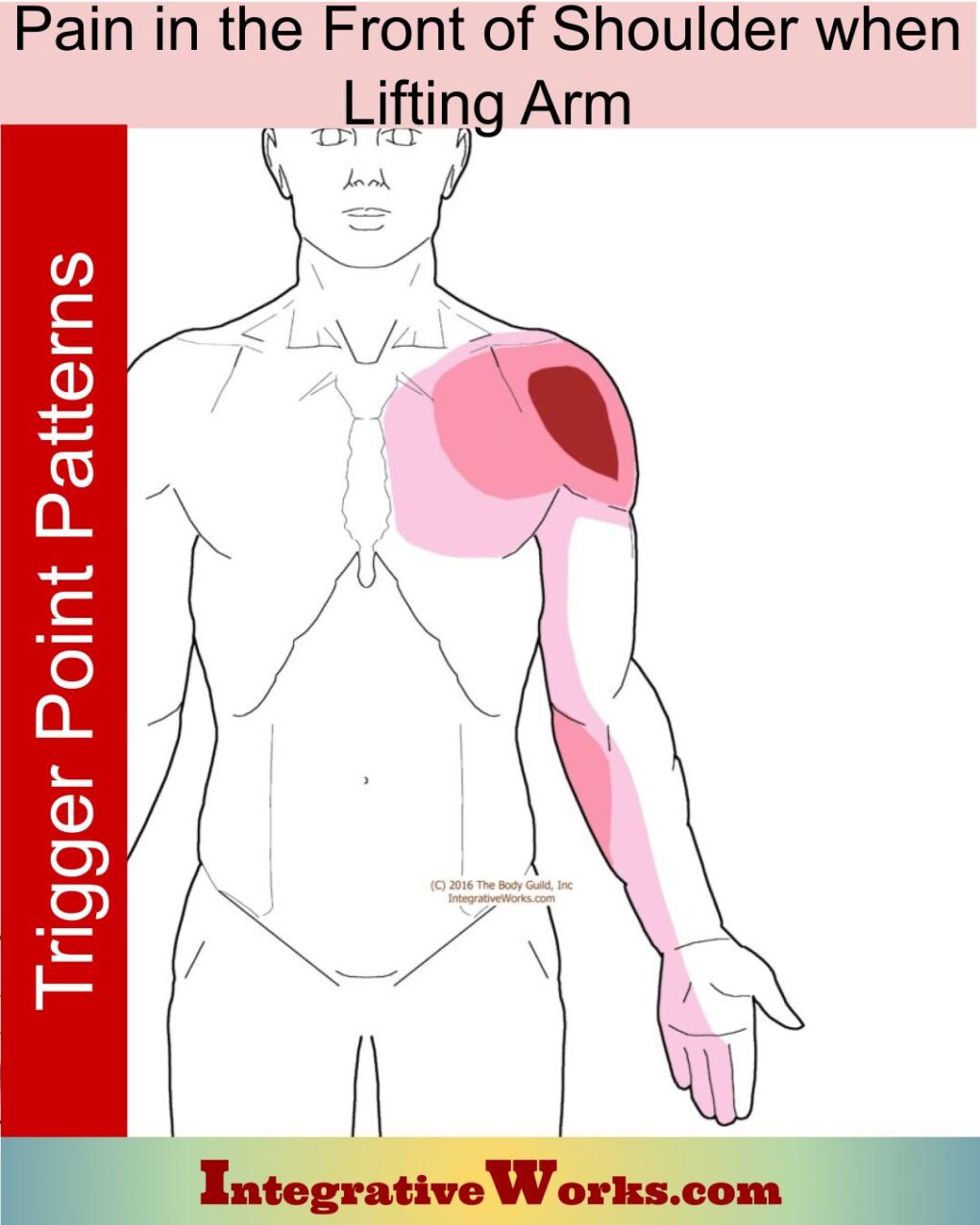
Pain in the Front of Shoulder When Lifting Arm
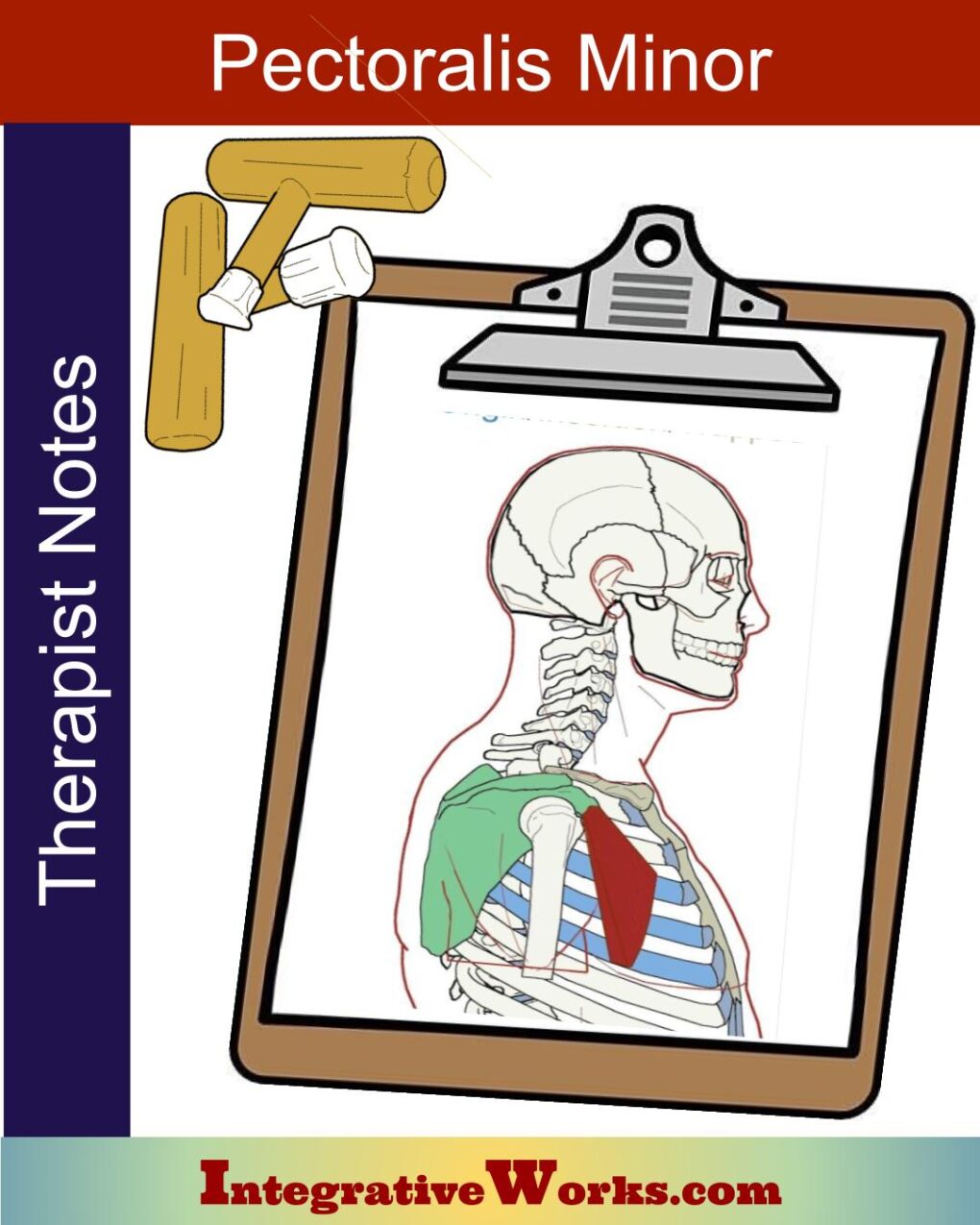
Pectoralis Minor – Massage Therapy Notes
Pectoralis Minor – Functional Anatomy
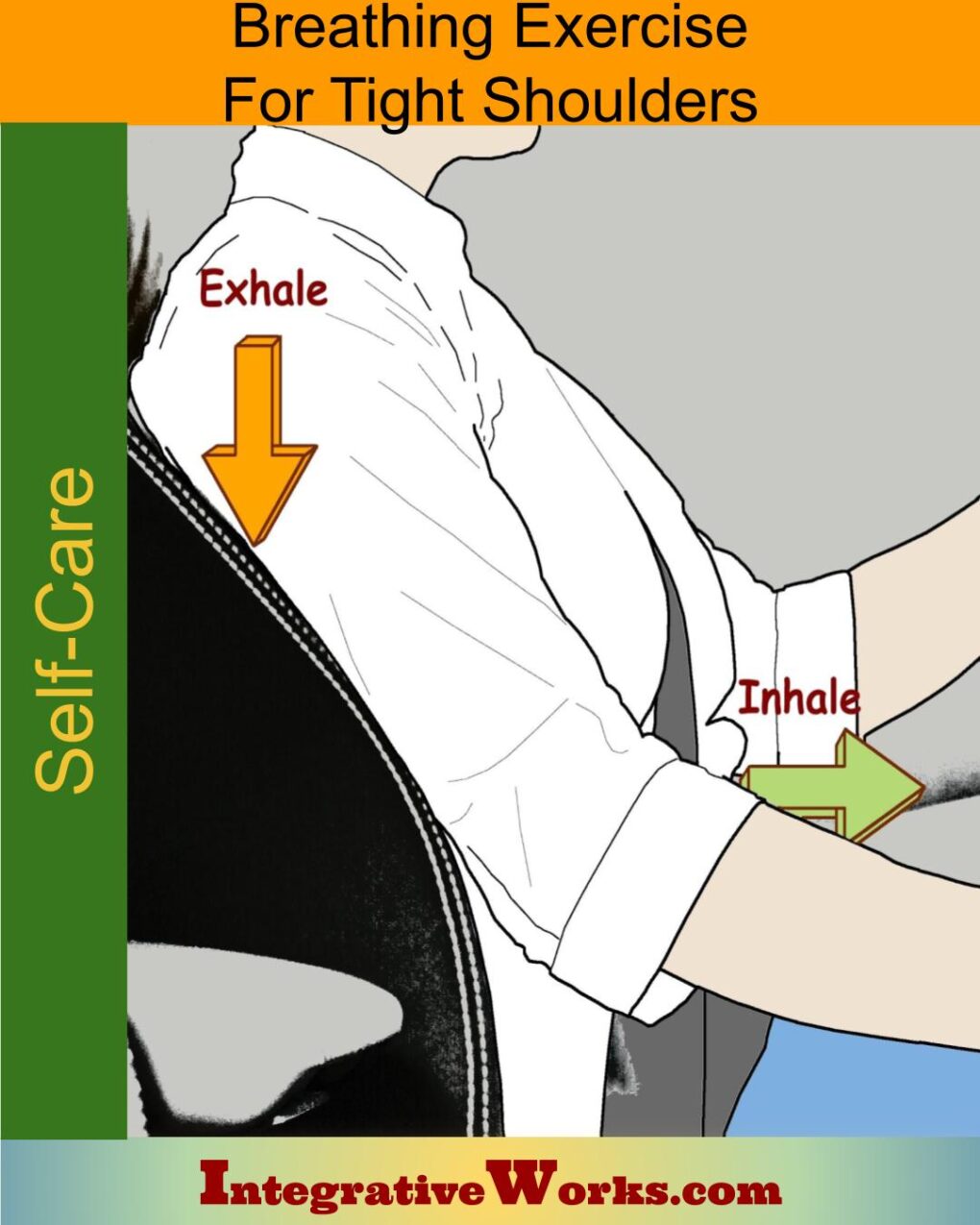
Self Care – Breathing Exercises to Reduce Shoulder Tension

Self Care – Doorway Stretches for Chest Muscles
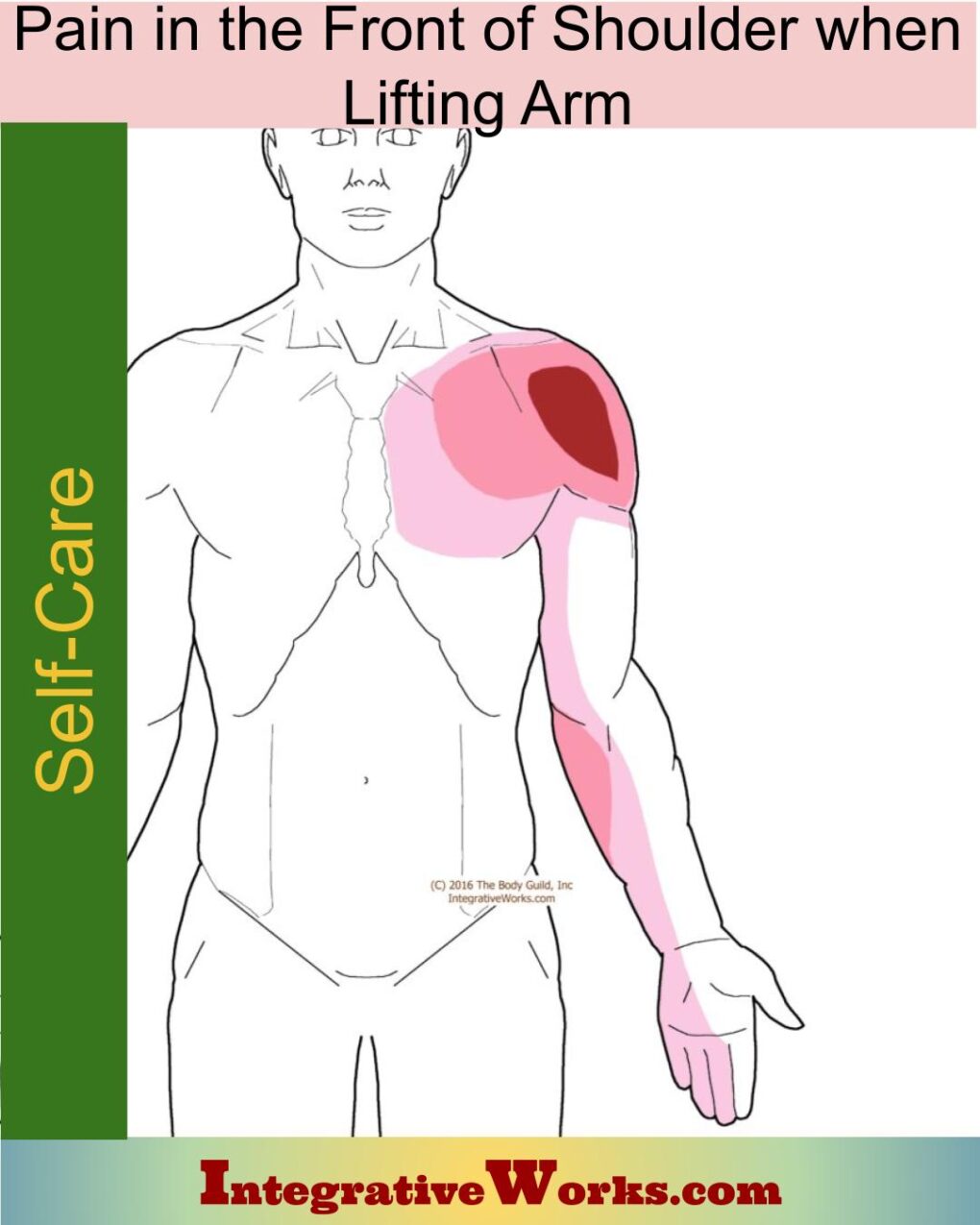
Self Care – Pain in the Front of Shoulder When Lifting Arm
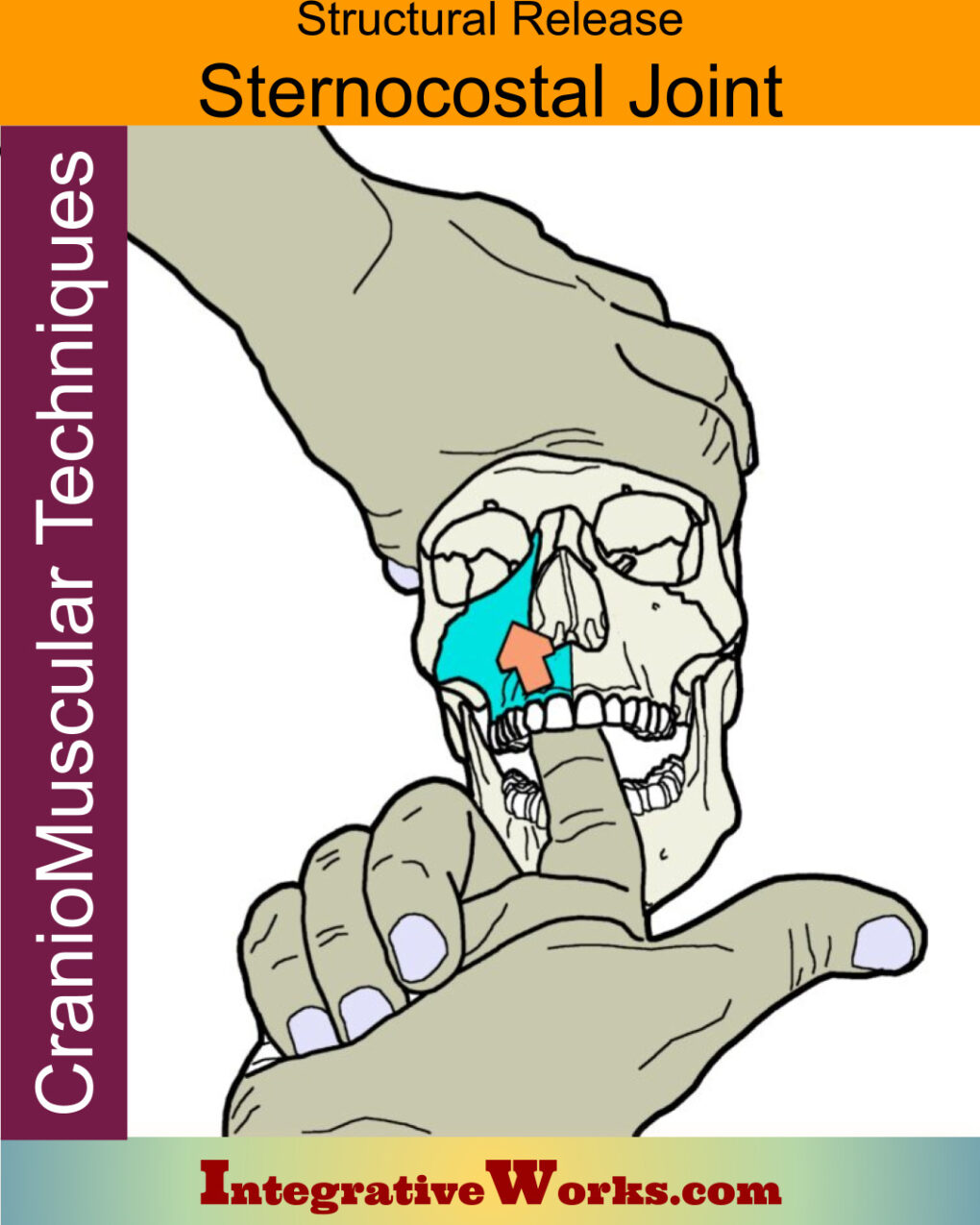
Sternocostal Joint – Structural Release
Thoracic Outlet – Functional Anatomy
Support Integrative Works to
stay independent
and produce great content.
You can subscribe to our community on Patreon. You will get links to free content and access to exclusive content not seen on this site. In addition, we will be posting anatomy illustrations, treatment notes, and sections from our manuals not found on this site. Thank you so much for being so supportive.

Cranio Cradle Cup
This mug has classic, colorful illustrations of the craniosacral system and vault hold #3. It makes a great gift and conversation piece.
Tony Preston has a practice in Atlanta, Georgia, where he sees clients. He has written materials and instructed classes since the mid-90s. This includes anatomy, trigger points, cranial, and neuromuscular.
Question? Comment? Typo?
integrativeworks@gmail.com
Interested in a session with Tony?
Call 404-226-1363
Follow us on Instagram
*This site is undergoing significant changes. We are reformatting and expanding the posts to make them easier to read. The result will also be more accessible and include more patterns with better self-care. Meanwhile, there may be formatting, content presentation, and readability inconsistencies. Until we get older posts updated, please excuse our mess.