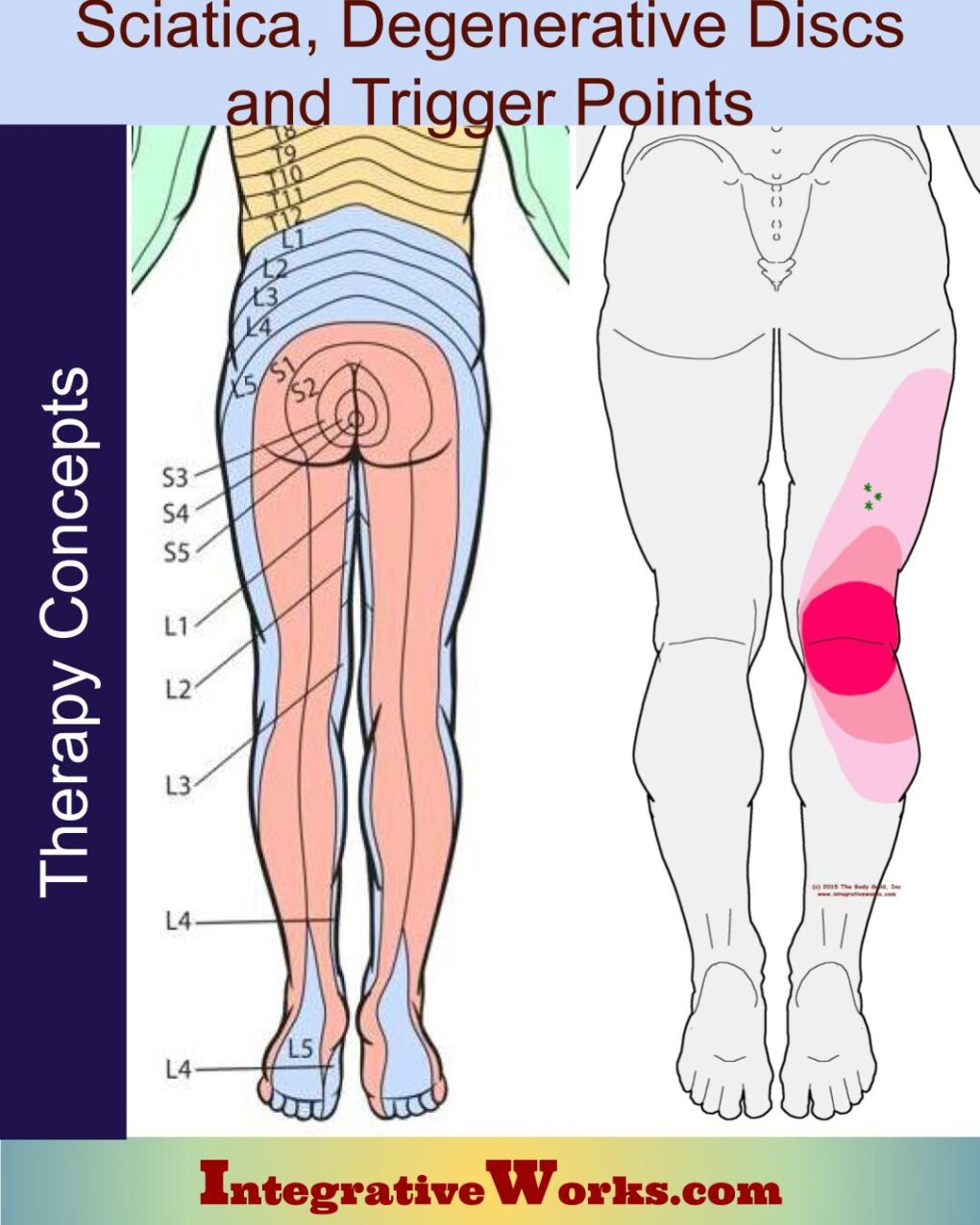
Many clients come to me with pain that their doctor has called “sciatica.” Sciatica originally referred to painful inflammation of the sciatic nerve. The sciatic nerve emerges from the lower lumbar vertebrae and upper sacral segments (L4-S3) and innervates the majority of the gluteal region, posterior thigh, and the lower leg. “Sciatica” is now commonly used to refer to any pain extending down in the back of the hip and leg.
Clients often report that they have Degenerative Disc Disease and may have had an MRI that shows that they have thin or bulging discs. I seldom find that the pattern of pain is connected to nerve root pressure at the spine as “Degenerative Disc Disease” would imply. When they describe the pain, I almost always identify a trigger point and can elicit the pain pattern by pressing on the trigger point nodule in the muscle or relieve the pain by releasing the trigger point.
Trigger Point assessment can lead to treatment approaches that are more direct, more effective, less invasive, and less expensive than other methods. Other methods of assessment have their strengths, but without trigger point assessment, the treatments are often prolonged or ineffective. Most of my new clients who come to me with “sciatica” have already been down that route.
Differences in
Trigger Point Referral (TPR) and
Nerve Root Pressure (NRP)
TPR/NRP usually have a different type of sensation
People describe nerve pressure as
- “that funny-bone electric shock feeling” or
- “like there is a nail driving into my muscle, especially when I move my spine like this” or
- “like there is something over the skin and I can’t feel it in my leg when I touch my leg with my hand.”
People describe trigger point referral as
- “muscle pain” or
- “that tingly falling asleep feeling, but I can feel it when I touch the skin.”
- Athletes often refer to trigger point pain as “tightness.”
- Yoga instructors and other stretch enthusiasts refer to trigger point referral as “that good stretch feeling.”
The description of the sensation cannot be used as a complete assessment.
TPR and NRP restrict your movement differently.
Trigger point research usually indicates the restriction of specific activities. Trigger points inhibit contraction and stretch within a particular band of a specific muscle. Because of that, they create specific changes in movement patterns.
- Trigger points of the rectus femoris produce buckling of the knee on stairs.
- Trigger points in the lateral hamstring produce pain in the back of the knee when getting up from a seated position.
- Trigger points in the gluteus medius create pain in the hip while seated for long periods.
- Trigger points in the supraspinatus create shoulder pain when brushing your teeth, or styling your hair.
The list goes on…
Nerve pressure is usually not usually directly connected to an activity. It may make the legs sluggish. It may make any movement involving that vertebra exquisitely painful. Sometimes nerve pressure will disable and atrophy a specific muscle. Usually, that happens when the nerve pressure is away from the spine.
Again, a more complete assessment is needed.
TPR and NRP have different patterns of sensation
Nerve root pressure in the lumbar vertebrae usually travels in a spiral around the hip and leg. Here are dermatome charts that show how nerve patterns run across legs.
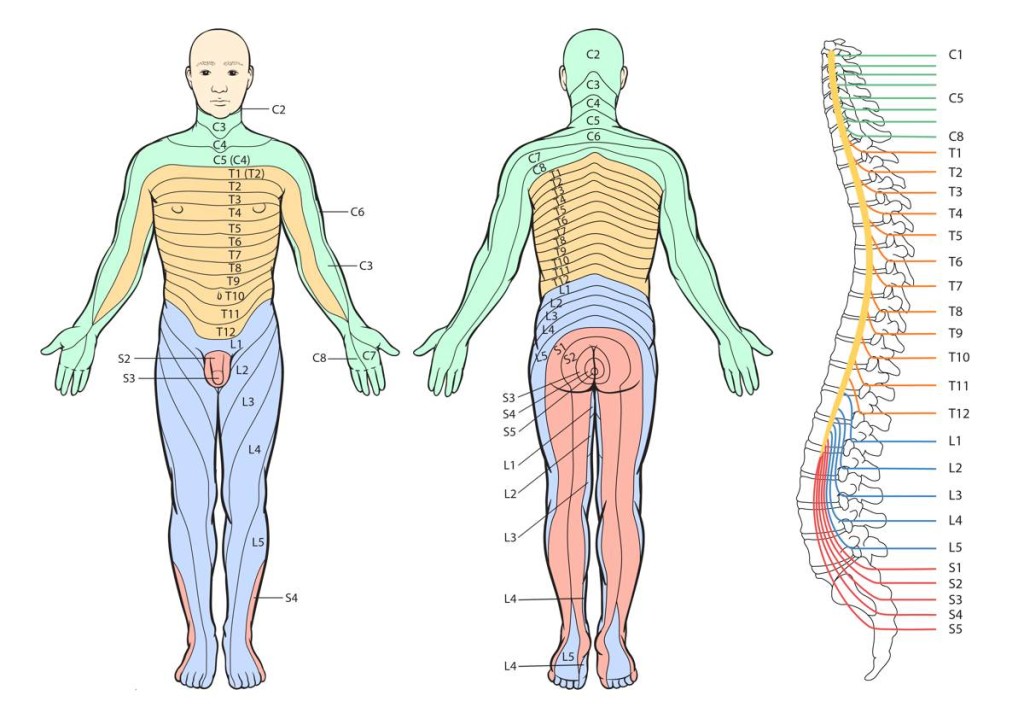
Dermatome patterns from the vertebral nerve roots. Note that the dermatomes that run straight down the legs are from sacral roots where there are no intervertebral discs to deteriorate.
Trigger point patterns in legs don’t spiral as nerve pressure patterns do. Trigger point patterns make no sense when looking at dermatome charts. The following are a few trigger point patterns that clients have been told are sciatica from degenerative disc problems.
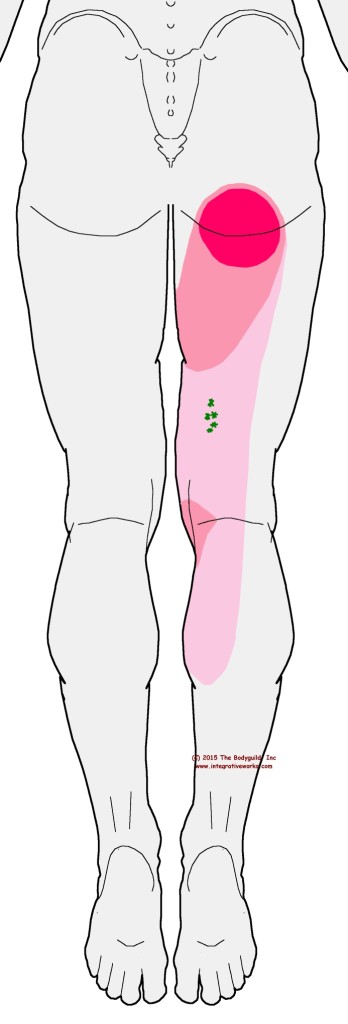
People with trigger points in the medial hamstring usually complain about a focus of pain right where they sit and, sometimes, tension down the back of the thigh. Some movements produce sharp pain at the inside of the knee.
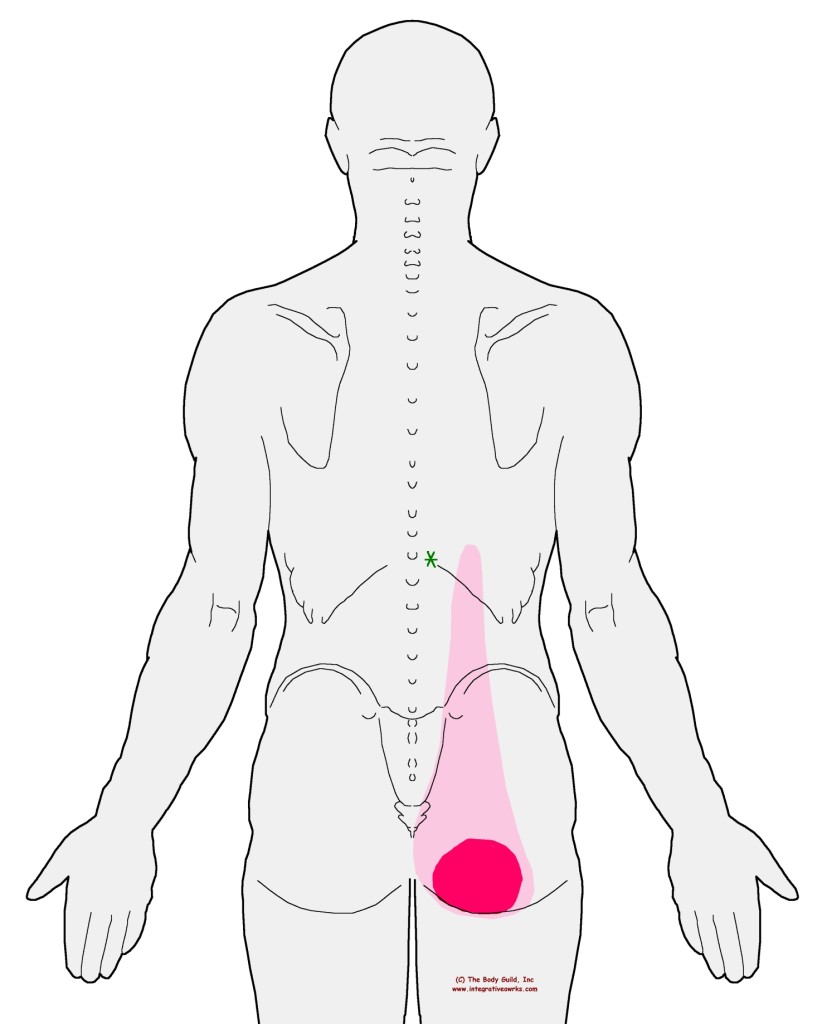
People with trigger points in the longissimus or medial hamstring have very similar complaints about where the pain is focused but very different complaints about the details of the pattern and when it hurts.
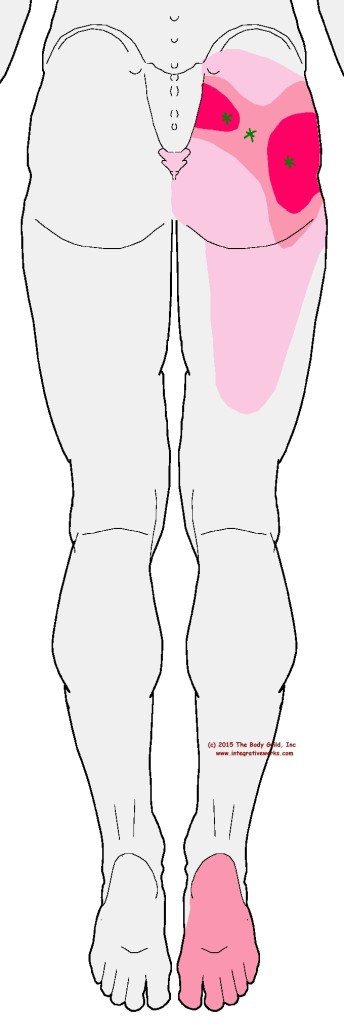
People with piriformis trigger points complain about pain across the hip and down the back of the thigh. It is often confused for sciatica. The “crawling” sensation on the bottom of the foot often accompanies this pattern or appears as its own symptom without the hip pain. By the way, the crawling pain on the bottom of the foot is nerve entrapment. The piriformis creates pressure on that nerve when the trigger point is active. It is included in most illustrations of the pattern because it often occurs with an active trigger point.
TPR and NRP pain can be elicited and relieved in different ways.
One of the tell-tale signs that I am dealing with trigger points is that the pain can be relieved with ice-and-stretch. In this case, I’ve done nothing to the nerve root at the spine. Also, It is obvious when I can elicit the pain with direct pressure on the trigger point. Nerve pressure at the spine responds to releasing restrictions around the vertebrae. Also, when the disc is severely compromised, the pain returns viciously upon standing.
Get help from the right professionals
I am not saying that you should see your doctor or a trigger point specialist. Instead, there is value in getting an assessment from both. Most of the new clients that I see with this kind of pain have already spoken with their doctor and are not satisfied with their care.
By the way, in new cases where the assessment indicates nerve pressure, I am very direct that the only responsible action, at that point, is to see a doctor for proper diagnosis and direction. Also, if your pain is severe and unfamiliar, even if you think it is a trigger point referral – see a doctor (orthopedist, chiropractor, neurologist) first.
Understanding the cause of the pain is an important step to finding an effective solution. I can usually assess, identify and release the trigger point quickly but the lasting solution to chronic pain is usually more involved. It may be about a series of sessions and/or a home program of stretching and strengthening. See your local massage and bodywork therapist for help with trigger points.
Support Integrative Works to
stay independent
and produce great content.
You can subscribe to our community on Patreon. You will get links to free content and access to exclusive content not seen on this site. In addition, we will be posting anatomy illustrations, treatment notes, and sections from our manuals not found on this site. Thank you so much for being so supportive.

Cranio Cradle Cup
This mug has classic, colorful illustrations of the craniosacral system and vault hold #3. It makes a great gift and conversation piece.
Tony Preston has a practice in Atlanta, Georgia, where he sees clients. He has written materials and instructed classes since the mid-90s. This includes anatomy, trigger points, cranial, and neuromuscular.
Question? Comment? Typo?
integrativeworks@gmail.com
Interested in a session with Tony?
Call 404-226-1363
Follow us on Instagram
*This site is undergoing significant changes. We are reformatting and expanding the posts to make them easier to read. The result will also be more accessible and include more patterns with better self-care. Meanwhile, there may be formatting, content presentation, and readability inconsistencies. Until we get older posts updated, please excuse our mess.