Sacroiliac Ligament – Functional Anatomy
This post is temporarily available to the public.
Support us & see more at IntegrativeWorks Patreon.
Overview
Here, you will find a bodyworker’s perspective on the anatomy of the sacroiliac ligament.
The sacroiliac ligament has three sections – anterior, interosseous, and posterior. Each section has a unique structure. Additionally, they impact the stability of the sacroiliac joint very differently.

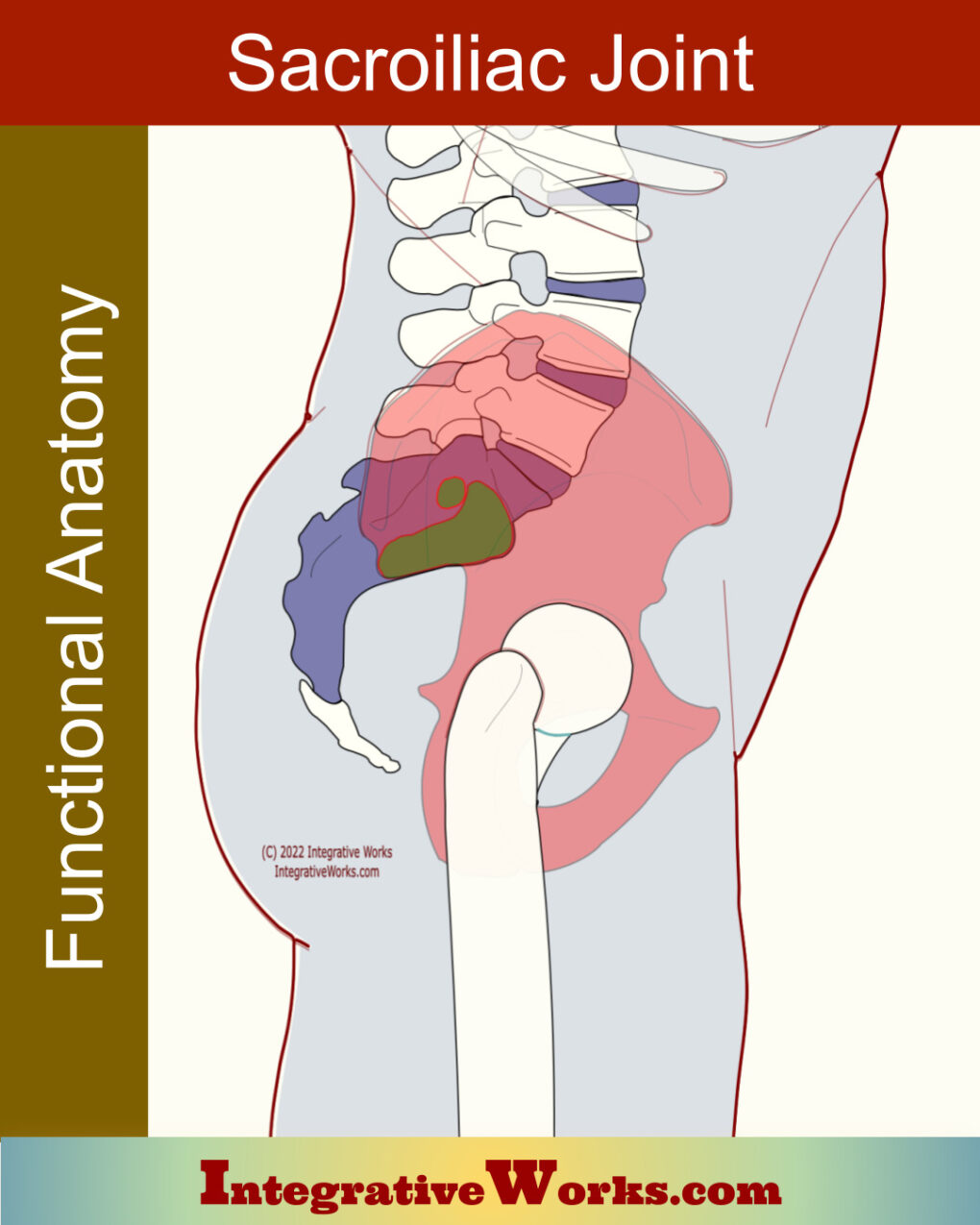
Sacroiliac Joint
The sacroiliac joint is a complicated and highly variable structure. Fortunately, it has probable differences based on age, sex, and race.
These variances can be important when trying to understand the likely structure in a particular case.
This post explores some of the studies around this variable joint.

Sacroiliac Ligament – Interosseus Section
The interosseus portion is the largest of ligaments supporting the sacroiliac joint. Some studies assert that it is the strongest ligament in the body. Additionally, it is the largest syndesmosis in the body.
This broad ligament attaches extensively to the lateral border of the sacrum alongside the first two or three sacral segments. Opposite, the other end attaches to the posterior ilium on the ischial tuberosity.
The interosseous sacroiliac ligament surrounds the dorsal and caudal borders of the joint. It lies deep to the posterior sacroiliac ligament. Additionally, it encloses any accessory sacroiliac joints.
It is surprisingly difficult to find an accurate, detailed cadaver or MRI of the ligament other than some cross-sections on the transverse plane. Possibly, because this ligament is deep in the space between the posterior ilium and the lateral sacrum. Further, the posterior sacroiliac ligament covers the interosseous portion, making it more difficult to reveal in cadaver photos.
Function
This interosseous portion restrains sacral flexion and axial rotation. Notably, it is the primary structure for providing stability to the sacroiliac joint.
Differences by Sex
This section of the sacroiliac ligament is commonly larger in females.

sacroiliac ligament – posterior view
Sacroiliac Ligament – Posterior
The posterior section is located over the deep depression between the ala of the sacrum and the PSIS, where the interosseous portion is.
This section has fibers that run almost laterally to connect the lateral posterior aspect of the upper two segments of the sacrum to the PSIS and the internal iliac crest. Shorter fibers in this area prevent the sacroiliac joint from flaring posteriorly. Longer fibers connect the 3rd and 4th sacral segments to the PSIS.
Superior fibers are blended with the fibers of the thoracolumbar fascia. Conversely, inferior fibers blend with the lateral sacrotuberous ligament.
Function
Of the different sections of the sacroiliac joint, it seems to have the greatest influence on the mobility of the sacroiliac joint.
Differences by Sex
The posterior sacroiliac section of the Sacroiliac ligament is commonly larger in males.

Sacroiliac Ligament – Anterior Section
Studies do not define this portion of the sacroiliac ligament as clearly as they describe other sections. Moreso, it doesn’t take much research to find conflicts in the details of those studies. For example, studies report that the interosseous section of this ligament encapsulates the caudal end of the joint. However, most illustrations show that the anterior section of this ligament veneers the caudal end of the joint.
This ligament is relatively thin along the ventral surface of the joint. Of the different sections of the sacroiliac joint, it seems to have the least influence on the stability of the sacroiliac joint. So, from another perspective, this is a thickening of the joint capsule. Consequently, its fragility leaves the capsule susceptible to ruptures that leak fluid over the nerves and other structures in that area.
Differences by Sex
This section of the Sacroiliac ligament is commonly larger in males.
Support Integrative Works to
stay independent
and produce great content.
You can subscribe to our community on Patreon. You will get links to free content and access to exclusive content not seen on this site. In addition, we will be posting anatomy illustrations, treatment notes, and sections from our manuals not found on this site. Thank you so much for being so supportive.
Cranio Cradle Cup
This mug has classic, colorful illustrations of the craniosacral system and vault hold #3. It makes a great gift and conversation piece.
Tony Preston has a practice in Atlanta, Georgia, where he sees clients. He has written materials and instructed classes since the mid-90s. This includes anatomy, trigger points, cranial, and neuromuscular.
Question? Comment? Typo?
integrativeworks@gmail.com
Follow us on Instagram

*This site is undergoing significant changes. We are reformatting and expanding the posts to make them easier to read. The result will also be more accessible and include more patterns with better self-care. Meanwhile, there may be formatting, content presentation, and readability inconsistencies. Until we get older posts updated, please excuse our mess.